

A systematic review on the effectiveness of robot-assisted minimally invasive gastrectomy
- PMID: 38990413
- PMCID: PMC11335791
- DOI: 10.1007/s10120-024-01534-1
A systematic review on the effectiveness of robot-assisted minimally invasive gastrectomy
Abstract
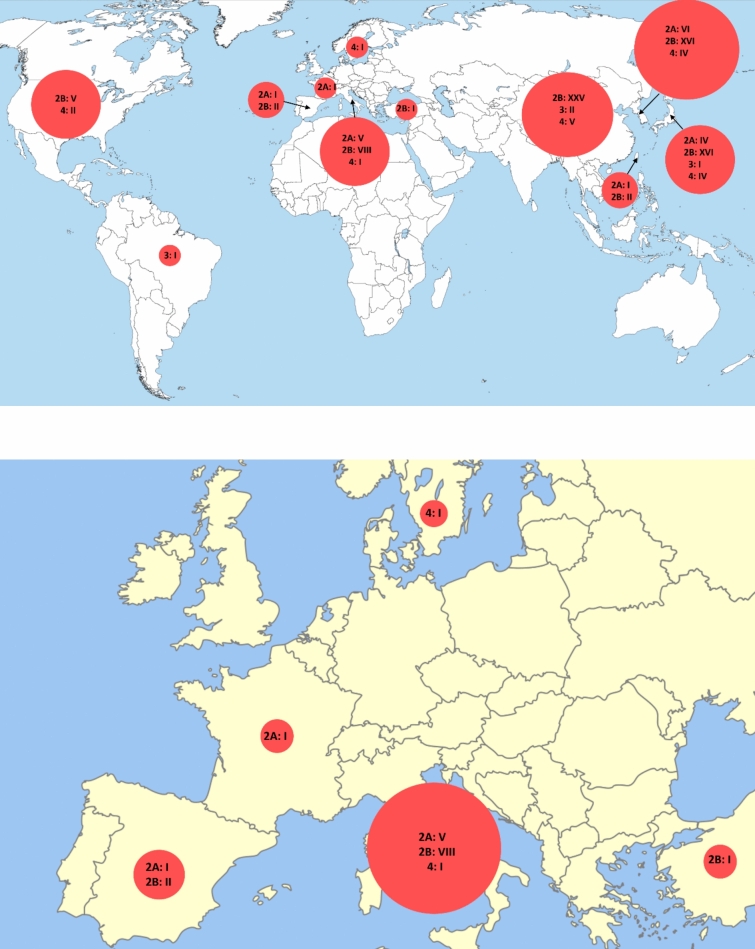
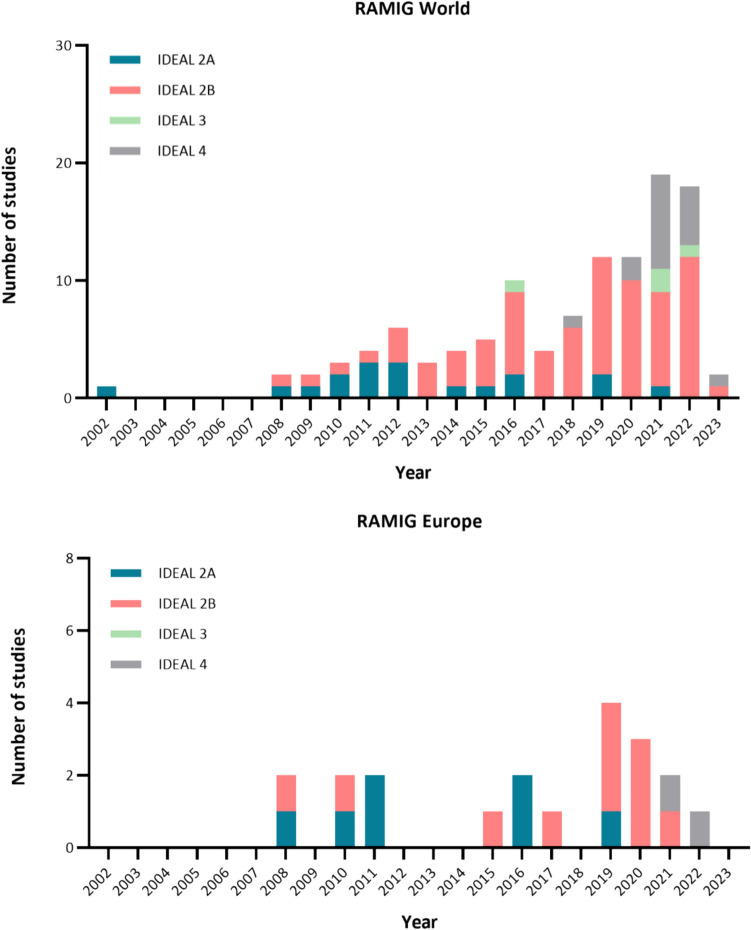
Background: Robot-assisted minimally invasive gastrectomy (RAMIG) is increasingly used as a surgical approach for gastric cancer. This study assessed the effectiveness of RAMIG and studied which stages of the IDEAL-framework (1 = Idea, 2A = Development, 2B = Exploration, 3 = Assessment, 4 = Long-term follow-up) were followed.
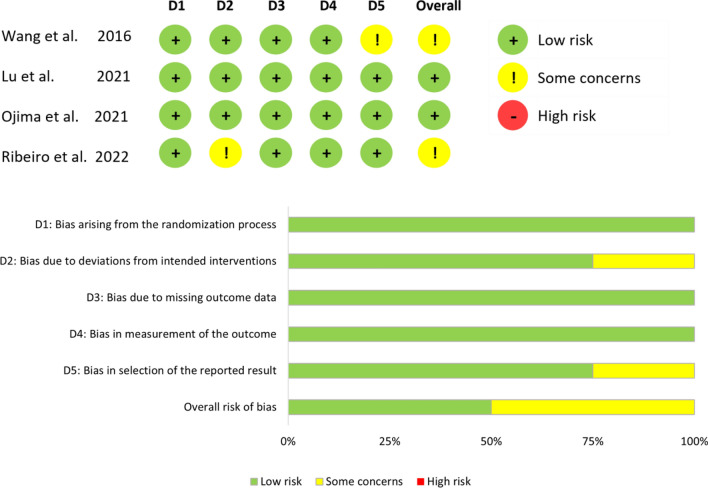
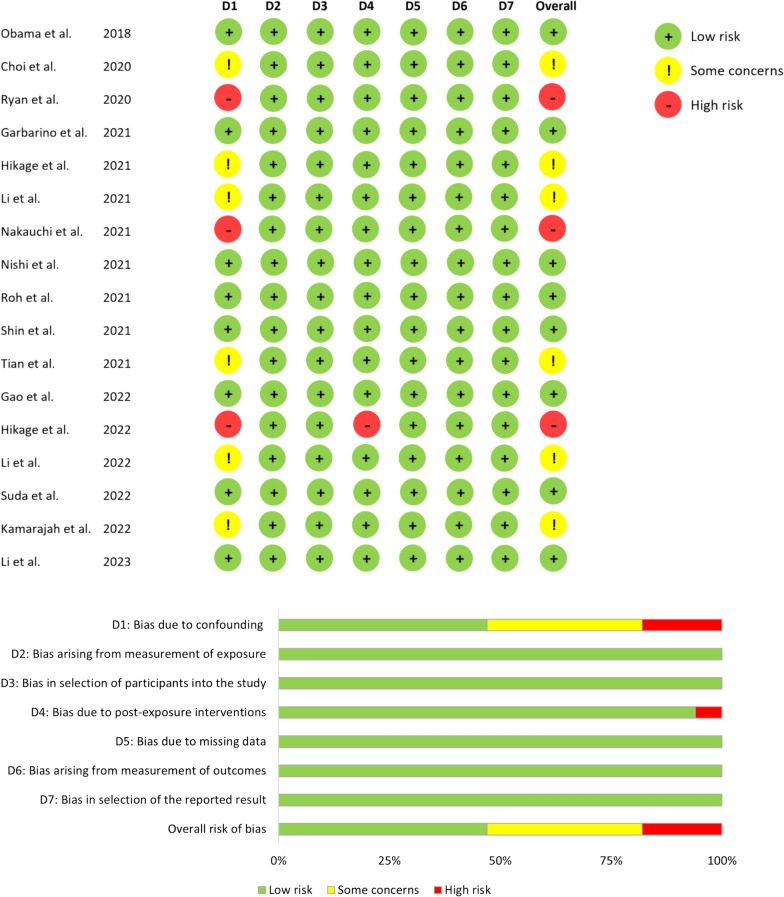
Methods: The Cochrane Library, Embase, Pubmed, and Web of Science were searched for studies on RAMIG up to January 2023. Data collection included the IDEAL-stage, demographics, number of participants, and study design. For randomized controlled trials (RCTs) and long-term studies, data on intra-, postoperative, and oncologic outcomes, survival, and costs of RAMIG were collected and summarized.
Results: Of the 114 included studies, none reported the IDEAL-stage. After full-text reading, 18 (16%) studies were considered IDEAL-2A, 75 (66%) IDEAL-2B, 4 (4%) IDEAL-3, and 17 (15%) IDEAL-4. The IDEAL-stages were followed sequentially (2A-4), with IDEAL-2A studies still ongoing. IDEAL-3 RCTs showed lower overall complications (8.5-9.2% RAMIG versus 17.6-19.3% laparoscopic total/subtotal gastrectomy), equal 30-day mortality (0%), and equal length of hospital stay for RAMIG (mean 5.7-8.5 days RAMIG versus 6.4-8.2 days open/laparoscopic total/subtotal gastrectomy). Lymph node yield was similar across techniques, but RAMIG incurred significantly higher costs than laparoscopic total/subtotal gastrectomy ($13,423-15,262 versus $10,165-10,945). IDEAL-4 studies showed similar or improved overall/disease-free survival for RAMIG.
Conclusion: During worldwide RAMIG implementation, the IDEAL-framework was followed in sequential order. IDEAL-3 and 4 long-term studies showed that RAMIG is similar or even better to conventional surgery in terms of hospital stay, lymph node yield, and overall/disease-free survival. In addition, RAMIG showed reduced postoperative complication rates, despite higher costs.
Keywords: Gastric Cancer; IDEAL-framework; Implementation; RAMIG; Robot-assisted gastrectomy.
© 2024. The Author(s).
Conflict of interest statement
Figures

References
-
- Al-Batran SE, Homann N, Pauligk C, Goetze TO, Meiler J, Kasper S, et al. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): a randomised, phase 2/3 trial. The Lancet. 2019;393(10184):1948–57.10.1016/S0140-6736(18)32557-1 - DOI - PubMed
-
- Kitano S, Iso Y, Moriyama M, Sugimachi K. Laparoscopy-assisted billroth I gastrectomy. Surg Laparosc Endosc. 1994;4(2):146–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
