

Blockade of IL1β and PD1 with Combination Chemotherapy Reduces Systemic Myeloid Suppression in Metastatic Pancreatic Cancer with Heterogeneous Effects in the Tumor
- PMID: 38990554
- PMCID: PMC11369625
- DOI: 10.1158/2326-6066.CIR-23-1073
Blockade of IL1β and PD1 with Combination Chemotherapy Reduces Systemic Myeloid Suppression in Metastatic Pancreatic Cancer with Heterogeneous Effects in the Tumor
Abstract
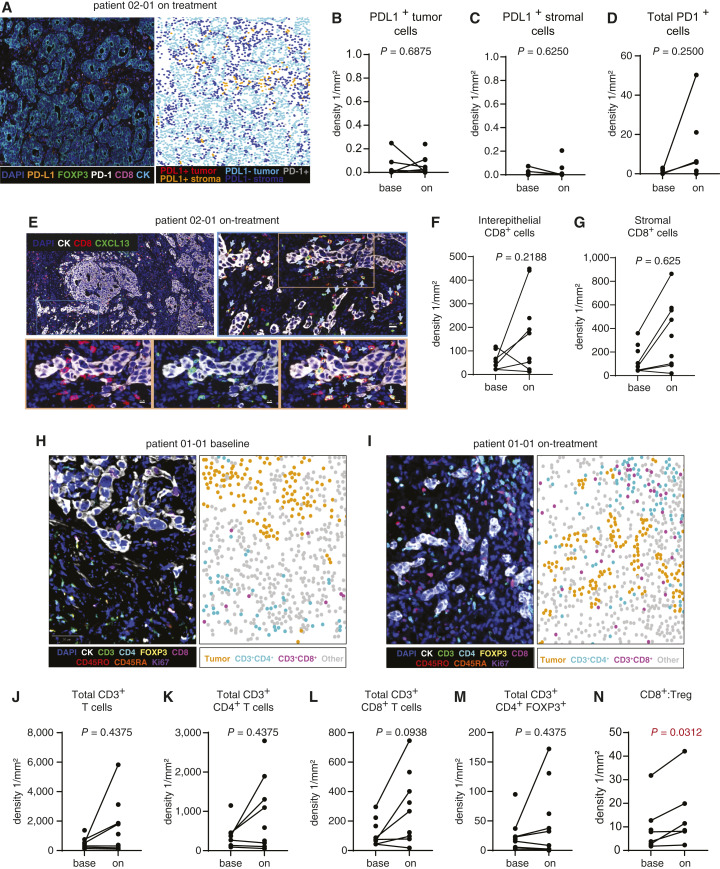
Innate inflammation promotes tumor development, although the role of innate inflammatory cytokines in established human tumors is unclear. Herein, we report clinical and translational results from a phase Ib trial testing whether IL1β blockade in human pancreatic cancer would alleviate myeloid immunosuppression and reveal antitumor T-cell responses to PD1 blockade. Patients with treatment-naïve advanced pancreatic ductal adenocarcinoma (n = 10) were treated with canakinumab, a high-affinity monoclonal human antiinterleukin-1β (IL1β), the PD1 blocking antibody spartalizumab, and gemcitabine/n(ab)paclitaxel. Analysis of paired peripheral blood from patients in the trial versus patients receiving multiagent chemotherapy showed a modest increase in HLA-DR+CD38+ activated CD8+ T cells and a decrease in circulating monocytic myeloid-derived suppressor cells (MDSC) by flow cytometry for patients in the trial but not in controls. Similarly, we used patient serum to differentiate monocytic MDSCs in vitro and showed that functional inhibition of T-cell proliferation was reduced when using on-treatment serum samples from patients in the trial but not when using serum from patients treated with chemotherapy alone. Within the tumor, we observed few changes in suppressive myeloid-cell populations or activated T cells as assessed by single-cell transcriptional profiling or multiplex immunofluorescence, although increases in CD8+ T cells suggest that improvements in the tumor immune microenvironment might be revealed by a larger study. Overall, the data indicate that exposure to PD1 and IL1β blockade induced a modest reactivation of peripheral CD8+ T cells and decreased circulating monocytic MDSCs; however, these changes did not lead to similarly uniform alterations in the tumor microenvironment.
©2024 The Authors; Published by the American Association for Cancer Research.
Conflict of interest statement
P.E. Oberstein reports other support from Novartis during the conduct of the study, as well as personal fees from Ipsen and Lilly outside the submitted work. O.E. Rahma reports personal fees from Merck, Celgene, Five Prime, GSK, Bayer, Roche/Genentech, Puretech, Imvax, Sobi, Boehringer Ingelheim and hold pending patent for “Methods of using pembrolizumab and trebananib” outside the submitted work. O.E. Rahma is a full-time associate of AstraZeneca not during the time period of the submitted work. H. Singh reports grants from AstraZeneca and other support from Dewpoint Therapeutics, Merck Sharpe & Dohme, Dava Oncology, and UpToDate outside the submitted work. T.A. Abrams reports grants and personal fees from AstraZeneca and personal fees from Eisai, Elevar, HistoSonics, and Sirtex outside the submitted work. J.M. Cleary reports personal fees from Blueprint Medicines, Incyte, and AstraZeneca and grants from Amgen, Merus, Roche, Servier, BMS, Esperas Pharma, AstraZeneca, Merck, Pyxis Oncology, Arcus, and GSK outside the submitted work. B.M. Huffman reports personal fees from Lilly outside the submitted work. K.J. Perez reports personal fees from Ipsen, Novartis, and Lantheus outside the submitted work. D.A. Rubinson reports personal fees from Taiho, Sirtex, and Instylla outside the submitted work. B.L. Schlechter reports Agemis and Janssen outside the submitted work. R. Surana reports personal fees from Grupo Oncoclinicas and other support from DAVA Oncology outside the submitted work. M.B. Yurgelun reports grants from Janssen and personal fees from Nouscom and UpToDate outside the submitted work. K.M. Sullivan reports personal fees from Eli Lilly outside the submitted work. M. Dougan reports personal fees from Neoleukin, Genentech, Partner Therapeutics, SQZ Biotech, AzurRx, Eli Lilly, Mallinckrodt Pharmaceuticals, Aditum, Foghorn Therapeutics, Palleon, Sorriso Pharmaceuticals, Generate Biomedicines, Asher Bio, Alloy Therapeutics, Third Rock Ventures, DE Shaw Research, Agenus, Astellas, and Curie Bio and other support from Veravas, Monod Bio, Axxis Bio, and Cerberus Therapeutics outside the submitted work. M. Dajee is a full-time associate of Novartis Institute for Biomedical Research and reports other support from Novartis Cooperation outside the submitted work. M.R. Pelletier is a full-time associate of Novartis Institute for Biomedical Research. S. Nazeer is a full-time associate of Novartis Pharma AG and a member of the clinical study team. M. Squires is a full-time associate of Novartis Pharma AG. B.M. Wolpin reports personal fees from Mirati; grants from Novartis; grants and personal fees from Revolution Medicines and Harbinger; personal fees from GRAIL, Ipsen, EcoR1 Capital, Third Rock Ventures, and Agenus; and grants from AstraZeneca and Eli Lilly outside the submitted work. J.A. Nowak reports grants from Natera and personal fees from Leica Biosystems outside the submitted work. D.M. Simeone reports grants from Novartis during the conduct of the study; grants from Micronoma, Immunovia, ClearNote Health, Biological Dynamics, and Tempus; personal fees from ClearNote Health, Interpace, Merck & Co., Bayer, and FibroGen outside of the submitted work. S.K. Dougan reports grants from Novartis during the conduct of the study; grants from BMS and Takeda; personal fees and other support from Kojin Therapeutics; and other support from Axxis Bio outside the submitted work. No disclosures were reported by the other authors.
Figures





References
-
- Lowenfels AB, Maisonneuve P, Cavallini G, Ammann RW, Lankisch PG, Andersen JR, et al. Pancreatitis and the risk of pancreatic cancer. International Pancreatitis Study Group. N Engl J Med 1993;328:1433–7. - PubMed
-
- Baron JA, Cole BF, Sandler RS, Haile RW, Ahnen D, Bresalier R, et al. A randomized trial of aspirin to prevent colorectal adenomas. N Engl J Med 2003;348:891–9. - PubMed
-
- Sandler RS, Halabi S, Baron JA, Budinger S, Paskett E, Keresztes R, et al. A randomized trial of aspirin to prevent colorectal adenomas in patients with previous colorectal cancer. N Engl J Med 2003;348:883–90. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
