

Hepatocellular Carcinoma in Metabolic Dysfunction-Associated Steatotic Liver Disease
- PMID: 38990573
- PMCID: PMC11240192
- DOI: 10.1001/jamanetworkopen.2024.21019
Hepatocellular Carcinoma in Metabolic Dysfunction-Associated Steatotic Liver Disease
Abstract
Importance: In the US, hepatocellular carcinoma (HCC) has been the most rapidly increasing cancer since 1980, and metabolic dysfunction-associated steatotic liver disease (MASLD) is expected to soon become the leading cause of HCC.
Objective: To develop a prediction model for HCC incidence in a cohort of patients with MASLD.
Design, setting, and participants: This prognostic study was conducted among patients aged at least 18 years with MASLD, identified using diagnosis of MASLD using International Classification of Diseases, Ninth Revision (ICD-9) or International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10) diagnosis codes; natural language processing of radiology imaging report text, which identified patients who had imaging evidence of MASLD but had not been formally diagnosed; or the Dallas Steatosis Index, a risk equation that identifies individuals likely to have MASLD with good precision. Patients were enrolled from Kaiser Permanente Northern California, an integrated health delivery system with more than 4.6 million members, with study entry between January 2009 and December 2018, and follow-up until HCC development, death, or study termination on September 30, 2021. Statistical analysis was performed during February 2023 and January 2024.
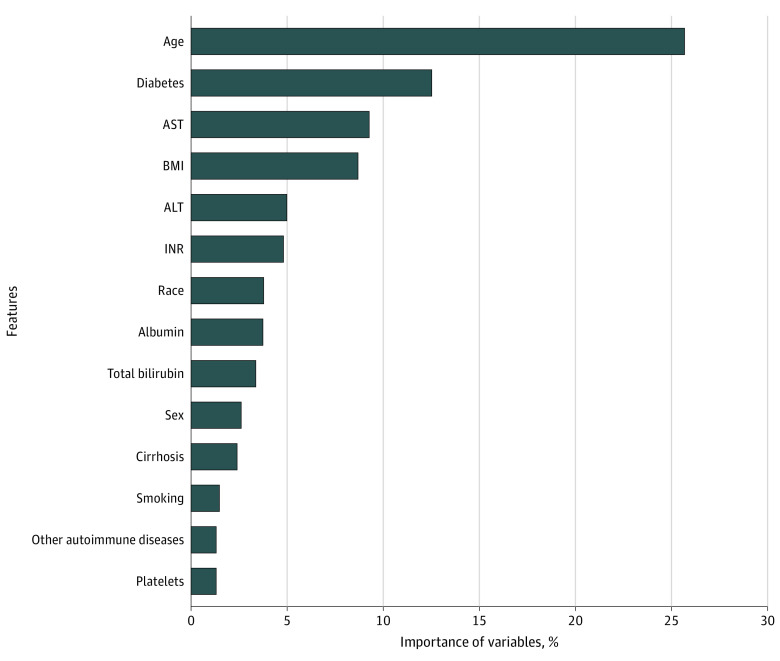
Exposure: Data were extracted from the electronic health record and included 18 routinely measured factors associated with MASLD.
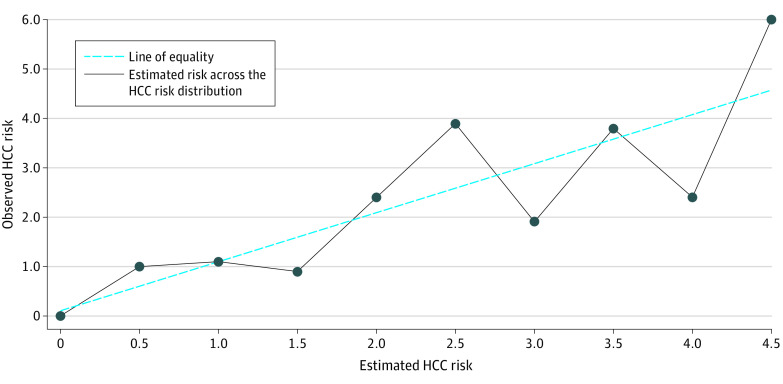
Main outcome and measures: The cohort was split (70:30) into derivation and internal validation sets; extreme gradient boosting was used to model HCC incidence. HCC risk was divided into 3 categories, with the cumulative estimated probability of HCC 0.05% or less classified as low risk; 0.05% to 0.09%, medium risk; and 0.1% or greater, high risk.
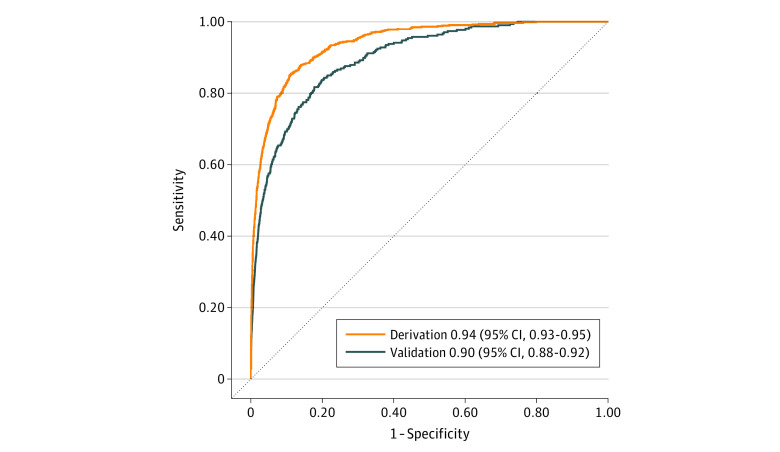
Results: A total of 1 811 461 patients (median age [IQR] at baseline, 52 [41-63] years; 982 300 [54.2%] female) participated in the study. During a median (range) follow-up of 9.3 (5.8-12.4) years, 946 patients developed HCC, for an incidence rate of 0.065 per 1000 person-years. The model achieved an area under the curve of 0.899 (95% CI, 0.882-0.916) in the validation set. At the medium-risk threshold, the model had a sensitivity of 87.5%, specificity of 81.4%, and a number needed to screen of 406. At the high-risk threshold, the model had a sensitivity of 78.4%, a specificity of 90.1%, and a number needed to screen of 241.
Conclusions and relevance: This prognostic study of more than 1.8 million patients with MASLD used electronic health record data to develop a prediction model to discriminate between individuals with and without incident HCC with good precision. This model could serve as a starting point to identify patients with MASLD who may need intervention and/or HCC surveillance.
Conflict of interest statement
Figures
Similar articles
-
Risk of de novo HCC in patients with MASLD following direct-acting antiviral-induced cure of HCV infection.J Hepatol. 2025 Apr;82(4):582-593. doi: 10.1016/j.jhep.2024.09.038. Epub 2024 Oct 3. J Hepatol. 2025. PMID: 39368711
-
Disease Progression for Histologic Diagnosis of Metabolic Dysfunction-Associated Steatotic Liver Disease in the Real-World: A Nationwide US Study.Dig Dis. 2025;43(1):36-45. doi: 10.1159/000541945. Epub 2024 Oct 14. Dig Dis. 2025. PMID: 39401491 Free PMC article.
-
Metabolic dysfunction-associated steatotic liver disease has become the most common cause of hepatocellular carcinoma in Sweden: A nationwide cohort study.Int J Cancer. 2025 Jan 1;156(1):40-51. doi: 10.1002/ijc.35097. Epub 2024 Jul 17. Int J Cancer. 2025. PMID: 39016032
-
Modifiable Risk Factors for Hepatocellular Carcinoma in Patients with Metabolic Dysfunction-Associated Steatotic Liver Disease: A Meta-Analysis.Am J Med. 2024 Nov;137(11):1072-1081.e32. doi: 10.1016/j.amjmed.2024.06.031. Epub 2024 Jul 22. Am J Med. 2024. PMID: 39047929
-
Phenotypes of Metabolic Dysfunction-Associated Steatotic Liver Disease-Associated Hepatocellular Carcinoma.Clin Gastroenterol Hepatol. 2024 Sep;22(9):1774-1789.e8. doi: 10.1016/j.cgh.2024.03.028. Epub 2024 Apr 10. Clin Gastroenterol Hepatol. 2024. PMID: 38604295 Review.
Cited by
-
The use of artificial intelligence in stereotactic ablative body radiotherapy for hepatocellular carcinoma.Front Med (Lausanne). 2025 Jun 6;12:1576494. doi: 10.3389/fmed.2025.1576494. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40547913 Free PMC article. Review.
-
Hepatic Iron Overload and Hepatocellular Carcinoma: New Insights into Pathophysiological Mechanisms and Therapeutic Approaches.Cancers (Basel). 2025 Jan 24;17(3):392. doi: 10.3390/cancers17030392. Cancers (Basel). 2025. PMID: 39941760 Free PMC article. Review.
-
Development of a Novel four-gene Model for Monitoring the Progression from Metabolic Dysfunction-associated Steatotic Liver Disease to Hepatocellular Carcinoma in Males.J Cancer. 2025 Jan 1;16(3):917-931. doi: 10.7150/jca.100724. eCollection 2025. J Cancer. 2025. PMID: 39781352 Free PMC article.
-
Role of Superb Microvascular Imaging (SMI) vascularity index values and vascularity patterns in the differential diagnosis of malignant liver lesions.Abdom Radiol (NY). 2025 Jun;50(6):2426-2439. doi: 10.1007/s00261-024-04711-z. Epub 2024 Nov 22. Abdom Radiol (NY). 2025. PMID: 39576317
-
Lipid Metabolism Reprogramming in Tumor-Associated Macrophages Modulates Their Function in Primary Liver Cancers.Cancers (Basel). 2025 May 31;17(11):1858. doi: 10.3390/cancers17111858. Cancers (Basel). 2025. PMID: 40507339 Free PMC article. Review.
References
-
- Howlader NNA, Krapcho M, Miller D, et al. . Cronin KA (eds). SEER Cancer Statistics Review, 1975-2016. Updated April 9, 2020. Accessed June 6, 2024. https://seer.cancer.gov/archive/csr/1975_2016/index.html
-
- Lobstein T, Jackson-Leach R, Powis J, Brinsden H, Gray M, eds. World Obesity Atlas 2023. World Obesity Federation; 2023.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
