

Randomized controlled trial reveals no benefit to a 3-month delay in COVID-19 mRNA booster vaccine
- PMID: 38990644
- PMCID: PMC11364387
- DOI: 10.1172/JCI181244
Randomized controlled trial reveals no benefit to a 3-month delay in COVID-19 mRNA booster vaccine
Abstract
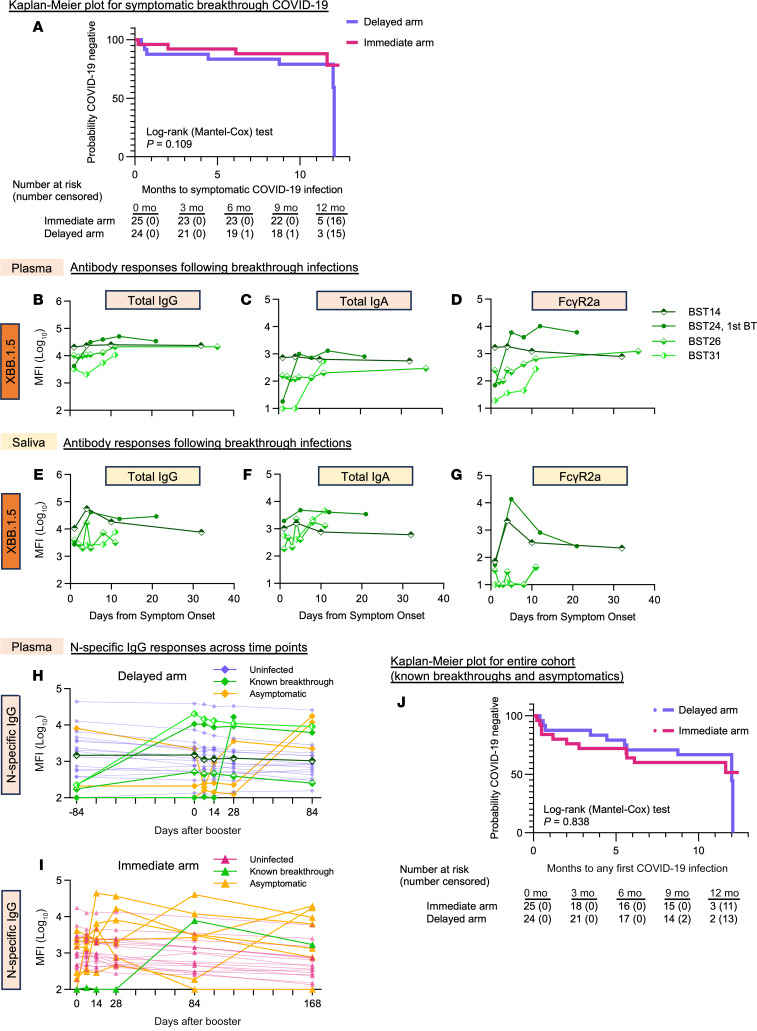
BACKGROUNDThere is uncertainty about the timing of booster vaccination against COVID-19 in highly vaccinated populations during the present endemic phase of COVID-19. Studies focused on primary vaccination have previously suggested improved immunity with a longer interval between the first and second vaccine doses.METHODSWe conducted a randomized, controlled trial (November 2022-August 2023) and assigned 52 fully vaccinated adults to an immediate or a 3-month delayed bivalent Spikevax mRNA booster vaccine. Follow-up visits were completed for 48 participants (n = 24 per arm), with collection of saliva and plasma samples following each visit.RESULTSThe rise in neutralizing antibody responses to ancestral and Omicron strains were almost identical between the immediate and delayed vaccination arms. Analyses of plasma and salivary antibody responses (IgG, IgA), plasma antibody-dependent phagocytic activity, and the decay kinetics of antibody responses were similar between the 2 arms. Symptomatic and asymptomatic SARS-CoV-2 infections occurred in 49% (21 of 49) participants over the median 11.5 months of follow-up and were also similar between the 2 arms.CONCLUSIONSOur data suggest that there was no benefit in delaying COVID-19 mRNA booster vaccination in preimmune populations during the present endemic phase of COVID-19.TRIAL REGISTRATIONAustralian New Zealand Clinical Trials Registry number 12622000411741 (https://anzctr.org.au/Trial/Registration/TrialReview.aspx?ACTRN=12622000411741).FUNDINGNational Health and Medical Research Council, Australia (program grant App1149990) and Medical Research Future Fund (App2005544).
Keywords: Adaptive immunity; Antigen; COVID-19; Immunoglobulins; Vaccines.
Figures



References
-
- Tan CY, et al. Effectiveness of bivalent mRNA vaccines against medically attended symptomatic SARS-CoV-2 infection and COVID-19-related hospital admission among SARS-CoV-2-naive and previously infected individuals: a retrospective cohort study. Lancet Infect Dis. 2023;23(12):1343–1348. doi: 10.1016/S1473-3099(23)00373-0. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
