

Photographic grading to evaluate facial cleanliness and trachoma among children in Amhara region, Ethiopia
- PMID: 38991011
- PMCID: PMC11290635
- DOI: 10.1371/journal.pntd.0012257
Photographic grading to evaluate facial cleanliness and trachoma among children in Amhara region, Ethiopia
Abstract
Background: Promotion of facial cleanliness is recommended for the elimination of blinding trachoma, largely because of observational studies that have found an association between various measures of facial uncleanliness and trachoma. However, when a field grader assesses both facial cleanliness and trachoma, associations may be biased. Assessment of photographs of the face and conjunctiva by masked graders may provide a less biased estimate of the relationship between facial cleanliness and trachoma.
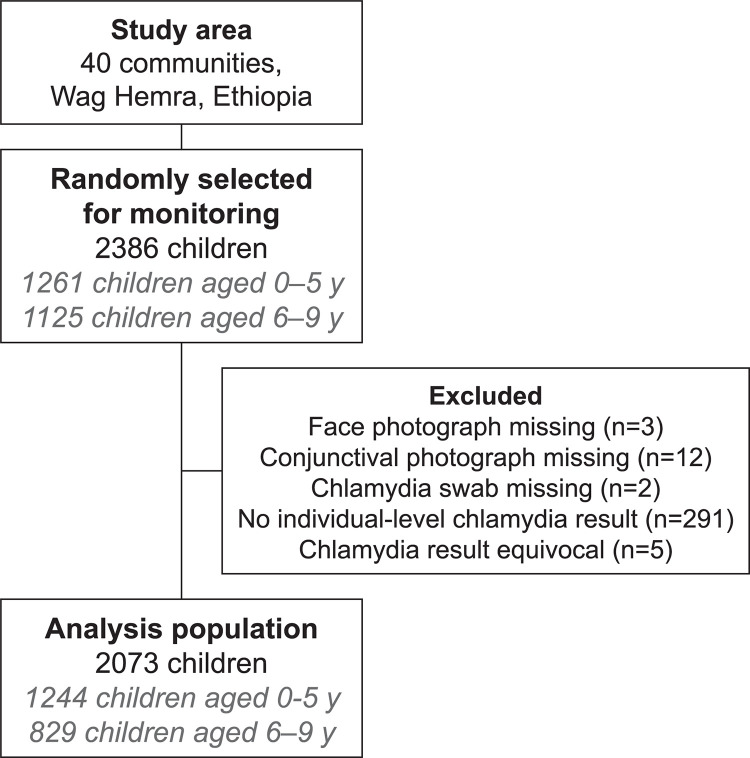
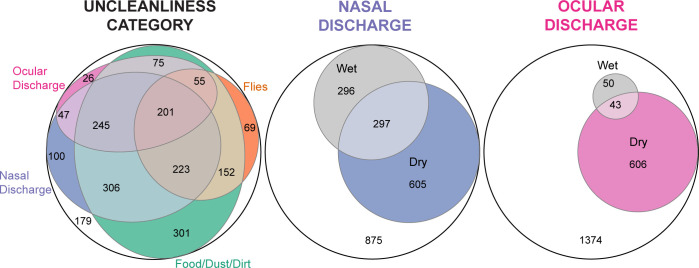
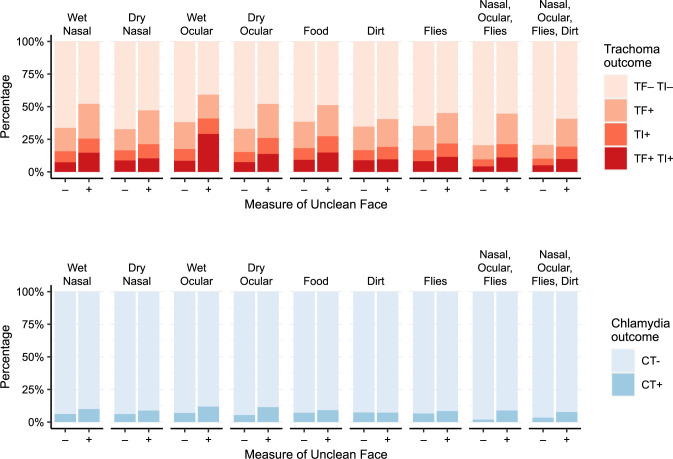
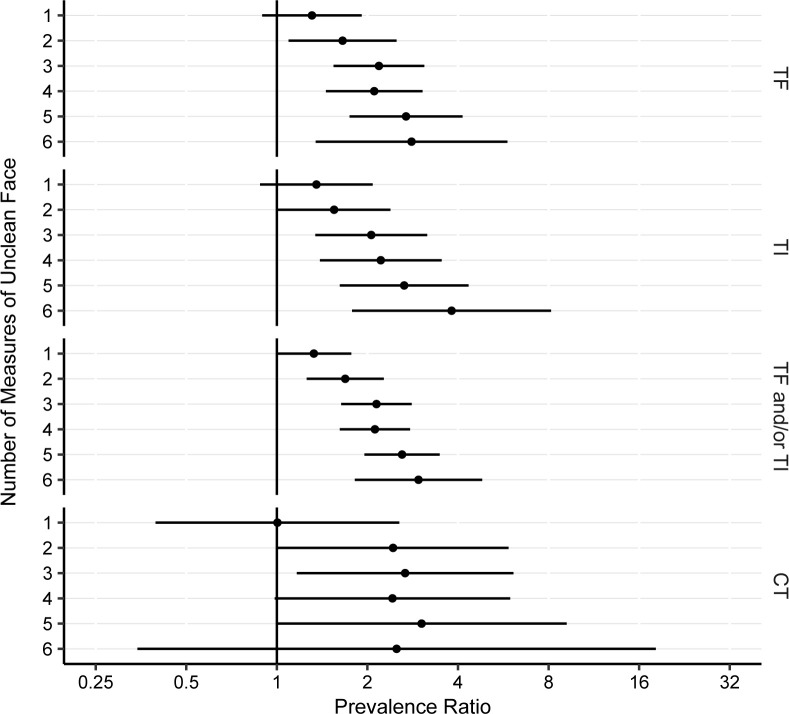
Methods: Face photographs, conjunctival photographs, and conjunctival swabs were obtained on a random sample of 0-9-year-old children from each of 40 communities in Amhara region, Ethiopia. Face photographs were assessed for the presence of seven measures of an unclean face (i.e., wet nasal discharge, dry nasal discharge, wet ocular discharge, dry ocular discharge, food, dust/dirt, and flies) by three independent masked photo-graders. Conjunctival photographs were similarly graded in a masked fashion for signs of clinically active trachoma. Conjunctival swabs were processed for Chlamydia trachomatis DNA.
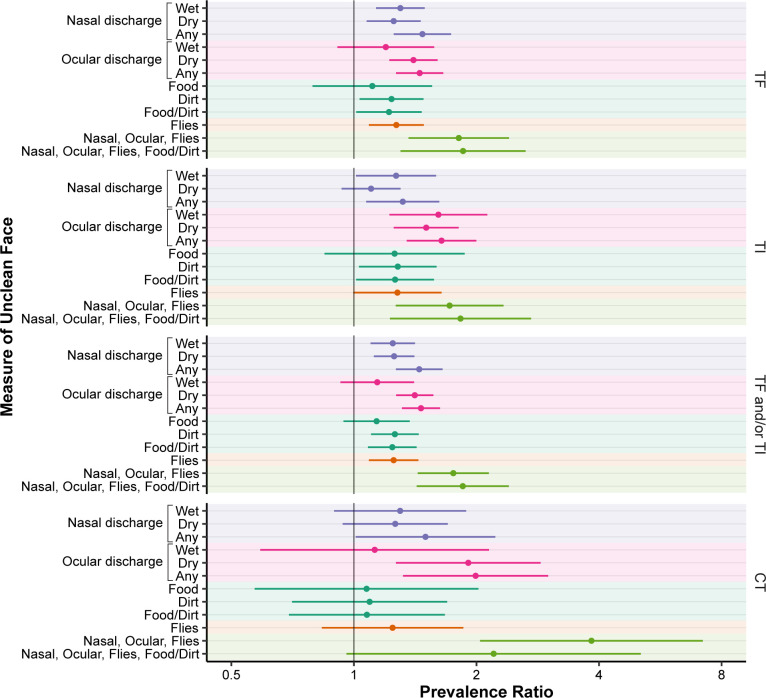
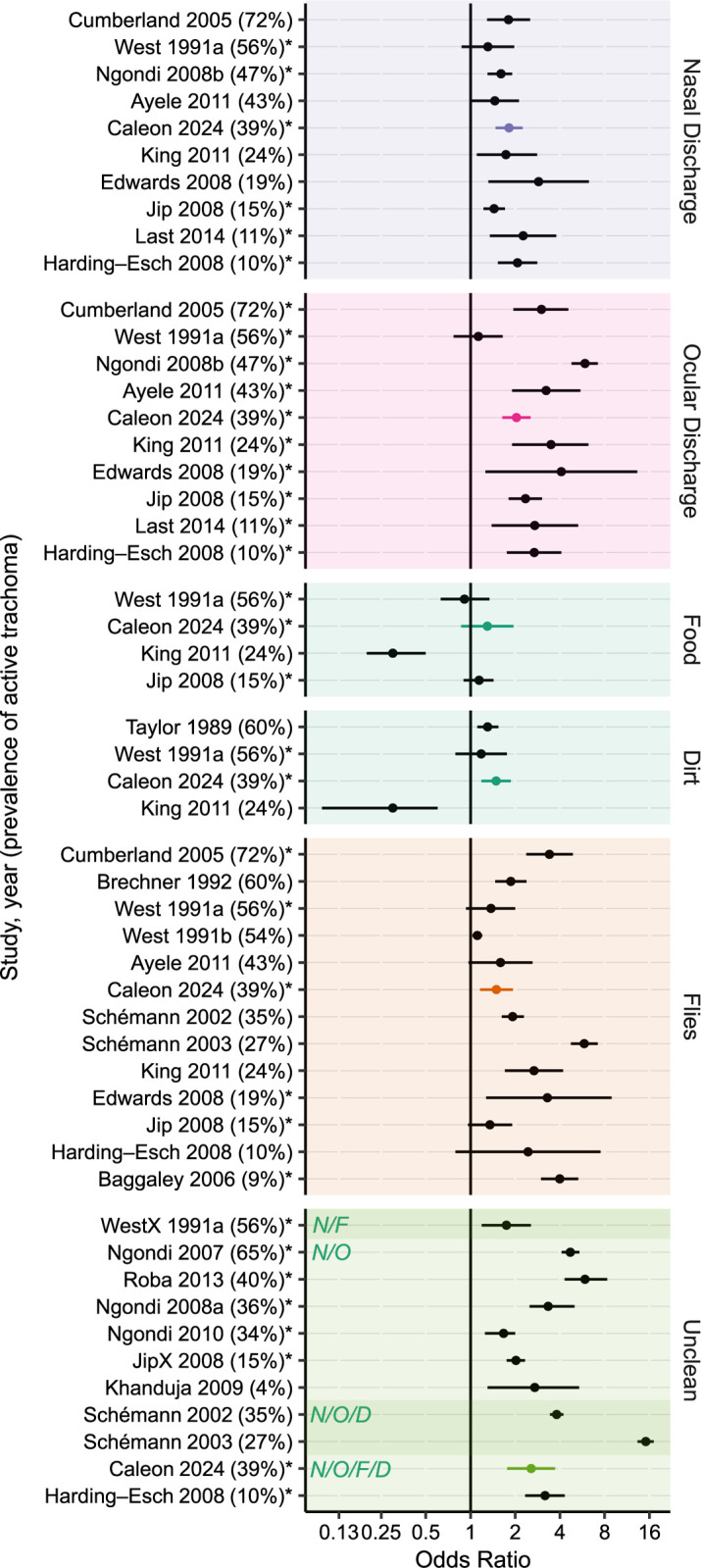
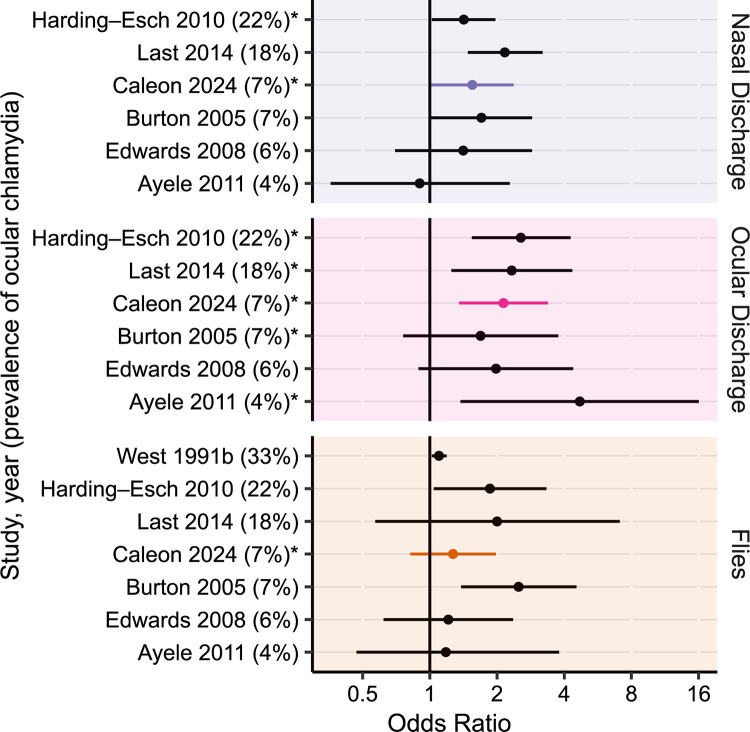
Results: Of 2073 children with complete data, 808 (39%) had evidence of clinically active trachoma, 150 (7%) had evidence of ocular chlamydia infection, and 2524 (91%) had at least one measure of an unclean face. Dry ocular discharge had the strongest association with clinically active trachoma (age- and sex-adjusted prevalence ratio [PR] 1.4, 95% CI 1.2-1.6) and ocular chlamydia infection (PR 1.9, 95%CI 1.3-2.9), although significant associations were observed between each of the measures of facial uncleanliness and trachoma.
Conclusions: Masked assessment of face and conjunctival photographs confirmed prior observational studies that have noted associations between various measures of facial uncleanliness and trachoma. The causal relationship between facial uncleanliness and trachoma is unclear since many features used to measure facial cleanliness (e.g., ocular discharge, nasal discharge, and flies) could be consequences of antecedent ocular chlamydia infection.
Trial registration: NCT02754583, clinicaltrials.gov.
Copyright: © 2024 Caleon et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Facial cleanliness indicators by time of day: results of a cross-sectional trachoma prevalence survey in Senegal.Parasit Vectors. 2020 Nov 18;13(1):556. doi: 10.1186/s13071-020-04410-w. Parasit Vectors. 2020. PMID: 33203456 Free PMC article.
-
Water, sanitation, and hygiene for control of trachoma in Ethiopia (WUHA): a two-arm, parallel-group, cluster-randomised trial.Lancet Glob Health. 2022 Jan;10(1):e87-e95. doi: 10.1016/S2214-109X(21)00409-5. Lancet Glob Health. 2022. PMID: 34919861 Free PMC article. Clinical Trial.
-
Cluster randomised controlled trial of double-dose azithromycin mass drug administration, facial cleanliness and fly control measures for trachoma control in Oromia, Ethiopia: the stronger SAFE trial protocol.BMJ Open. 2024 Dec 23;14(12):e084478. doi: 10.1136/bmjopen-2024-084478. BMJ Open. 2024. PMID: 39719287 Free PMC article.
-
Beyond the SAFE strategy: Systematic review and meta-analysis of prevalence and associated factors of active trachoma among children in Ethiopia.PLoS One. 2025 Feb 20;20(2):e0312024. doi: 10.1371/journal.pone.0312024. eCollection 2025. PLoS One. 2025. PMID: 39977409 Free PMC article.
-
Trachoma.Lancet. 2014 Dec 13;384(9960):2142-52. doi: 10.1016/S0140-6736(13)62182-0. Epub 2014 Jul 17. Lancet. 2014. PMID: 25043452 Review.
References
-
- Flaxman SR, Bourne RRA, Resnikoff S, Ackland P, Braithwaite T, Cicinelli MV, et al.. Global causes of blindness and distance vision impairment 1990–2020: a systematic review and meta-analysis. Lancet Glob Health. 2017;5(12):e1221–e34. Epub 2017/10/17. doi: 10.1016/S2214-109X(17)30393-5 . - DOI - PubMed
-
- World Health Organization. WHO alliance for the global elimination of trachoma: progress report on elimination of trachoma, 2022 2023. Available from: https://iris.who.int/bitstream/handle/10665/371095/WER9828-297-313.pdf.
-
- Solomon AW, World Health Organization., London School of Hygiene and Tropical Medicine., International Trachoma Initiative. Trachoma control: a guide for programme managers. Geneva: World Health Organization; 2006. 53 p. p.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
