

Machine Learning Model for Anesthetic Risk Stratification for Gynecologic and Obstetric Patients: Cross-Sectional Study Outlining a Novel Approach for Early Detection
- PMID: 38991090
- PMCID: PMC11375379
- DOI: 10.2196/54097
Machine Learning Model for Anesthetic Risk Stratification for Gynecologic and Obstetric Patients: Cross-Sectional Study Outlining a Novel Approach for Early Detection
Abstract
Background: Preoperative evaluation is important, and this study explored the application of machine learning methods for anesthetic risk classification and the evaluation of the contributions of various factors. To minimize the effects of confounding variables during model training, we used a homogenous group with similar physiological states and ages undergoing similar pelvic organ-related procedures not involving malignancies.
Objective: Data on women of reproductive age (age 20-50 years) who underwent gestational or gynecological surgery between January 1, 2017, and December 31, 2021, were obtained from the National Taiwan University Hospital Integrated Medical Database.
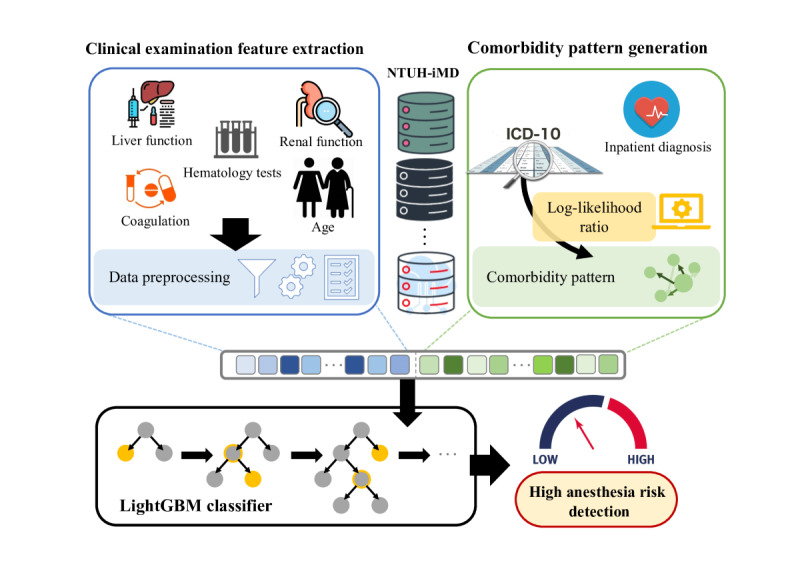
Methods: We first performed an exploratory analysis and selected key features. We then performed data preprocessing to acquire relevant features related to preoperative examination. To further enhance predictive performance, we used the log-likelihood ratio algorithm to generate comorbidity patterns. Finally, we input the processed features into the light gradient boosting machine (LightGBM) model for training and subsequent prediction.
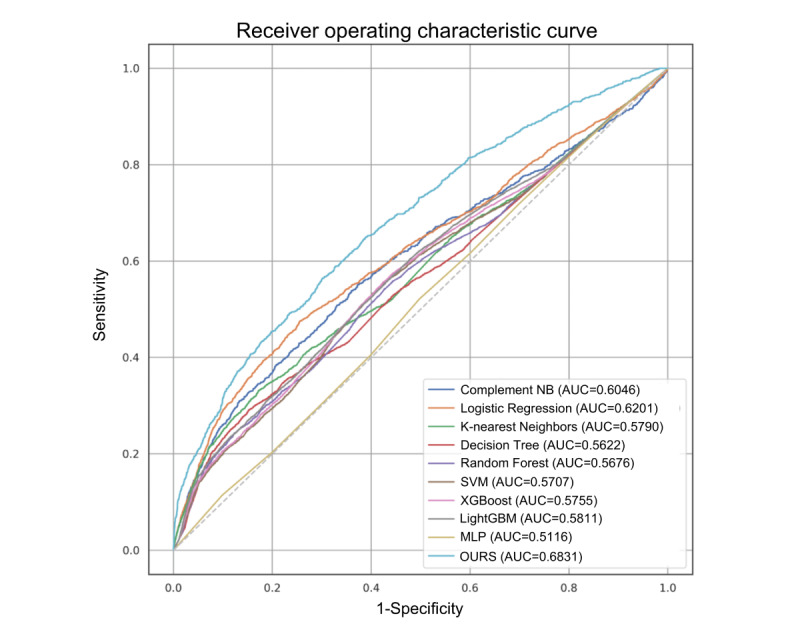
Results: A total of 10,892 patients were included. Within this data set, 9893 patients were classified as having low anesthetic risk (American Society of Anesthesiologists physical status score of 1-2), and 999 patients were classified as having high anesthetic risk (American Society of Anesthesiologists physical status score of >2). The area under the receiver operating characteristic curve of the proposed model was 0.6831.
Conclusions: By combining comorbidity information and clinical laboratory data, our methodology based on the LightGBM model provides more accurate predictions for anesthetic risk classification.
Trial registration: Research Ethics Committee of the National Taiwan University Hospital 202204010RINB; https://www.ntuh.gov.tw/RECO/Index.action.
Keywords: ASA classification; American Society of Anesthesiologists; anesthetic risk; artificial intelligence; clinical laboratory data; comorbidity; early detection; gestational; gradient boosting machine; gynecological and obstetric procedure; gynecology; laboratory data; machine learning; machine learning model; obstetrics; physiological; preoperative evaluation; risk; risk classification.
©Feng-Fang Tsai, Yung-Chun Chang, Yu-Wen Chiu, Bor-Ching Sheu, Min-Huei Hsu, Huei-Ming Yeh. Originally published in JMIR Formative Research (https://formative.jmir.org), 21.08.2024.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Hackett NJ, De Oliveira GS, Jain UK, Kim JYS. ASA class is a reliable independent predictor of medical complications and mortality following surgery. Int J Surg. 2015;18:184–190. doi: 10.1016/j.ijsu.2015.04.079. https://linkinghub.elsevier.com/retrieve/pii/S1743-9191(15)00206-X S1743-9191(15)00206-X - DOI - PubMed
-
- Benesch C, Glance LG, Derdeyn CP, Fleisher LA, Holloway RG, Messé SR, Mijalski C, Nelson MT, Power M, Welch BG. Perioperative neurological evaluation and management to lower the risk of acute stroke in patients undergoing noncardiac, nonneurological surgery: a scientific statement from the American Heart Association/American Stroke Association. Circulation. 2021;143(19):e923–e946. doi: 10.1161/CIR.0000000000000968. https://www.ahajournals.org/doi/abs/10.1161/CIR.0000000000000968?url_ver... - DOI - PubMed
LinkOut - more resources
Full Text Sources
