

Deep phenotyping of unaffected carriers of pathogenic BMPR2 variants screened for pulmonary arterial hypertension
- PMID: 38991711
- PMCID: PMC11447285
- DOI: 10.1183/13993003.00442-2024
Deep phenotyping of unaffected carriers of pathogenic BMPR2 variants screened for pulmonary arterial hypertension
Abstract
Introduction: Pathogenic variants in the gene encoding for BMPR2 are a major genetic risk factor for heritable pulmonary arterial hypertension. Owing to incomplete penetrance, deep phenotyping of unaffected carriers of a pathogenic BMPR2 variant through multimodality screening may aid in early diagnosis and identify susceptibility traits for future development of pulmonary arterial hypertension.
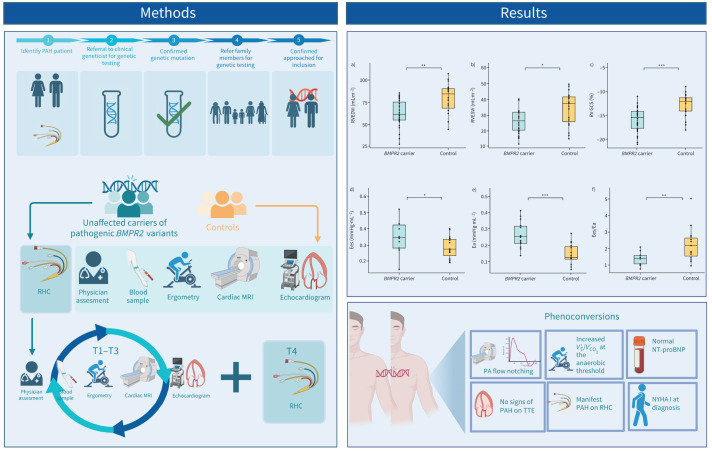
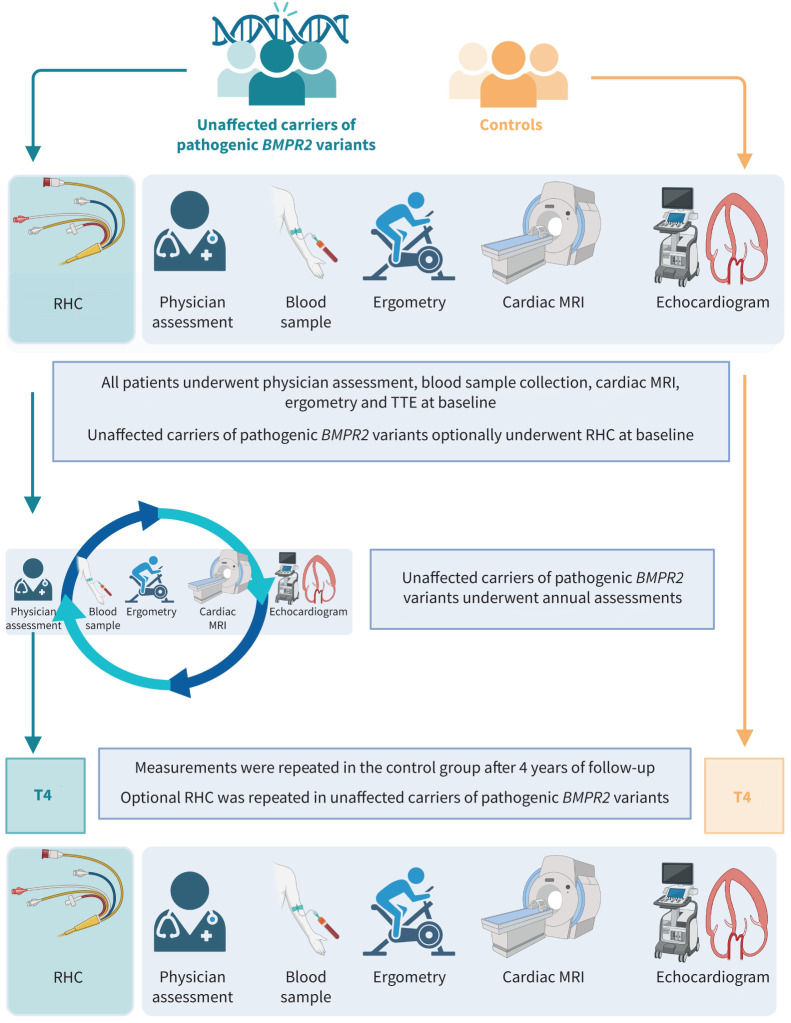
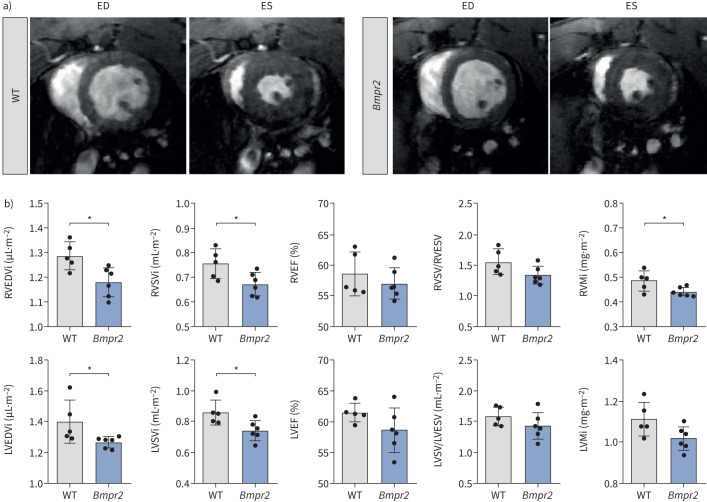
Methods: 28 unaffected carriers (44±16 years, 57% female) and 21 healthy controls (44±18 years, 48% female) underwent annual screening, including cardiac magnetic resonance imaging, transthoracic echocardiography, cardiopulmonary exercise testing and right heart catheterisation. Right ventricular pressure-volume loops were constructed to assess load-independent contractility and compared with a healthy control group. A transgenic Bmpr2Δ71Ex1/+ rat model was employed to validate findings from humans.
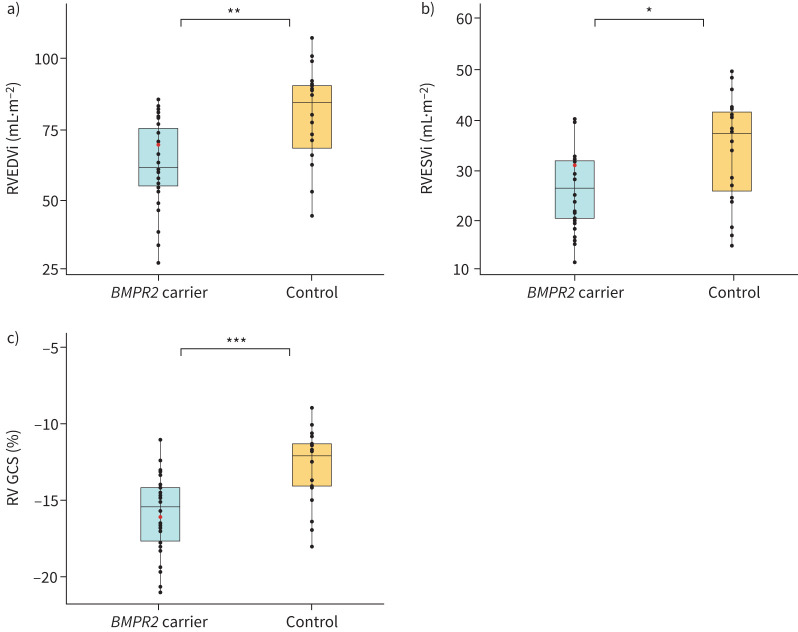
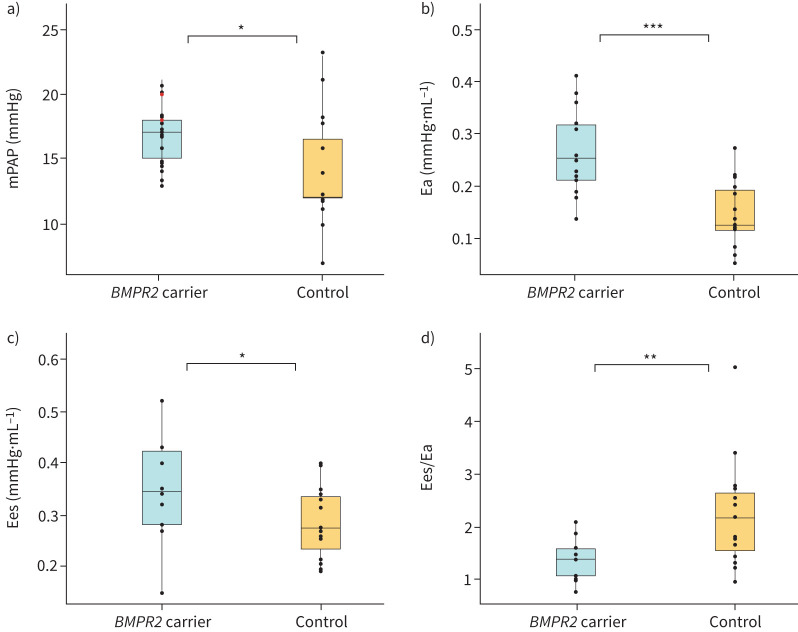
Results: Unaffected carriers had lower indexed right ventricular end-diastolic (79.5±17.6 mL·m-2 versus 62.7±15.3 mL·m-2; p=0.001), end-systolic (34.2±10.5 mL·m-2 versus 27.1±8.3 mL·m-2; p=0.014) and left ventricular end-diastolic (68.9±14.1 mL·m-2 versus 58.5±10.7 mL·m-2; p=0.007) volumes than control subjects. Bmpr2Δ71Ex1/+ rats were also observed to have smaller cardiac volumes than wild-type rats. Pressure-volume loop analysis showed that unaffected carriers had significantly higher afterload (arterial elastance 0.15±0.06 versus 0.27±0.08 mmHg·mL-1; p<0.001) and end-systolic elastance (0.28±0.07 versus 0.35±0.10 mmHg·mL-1; p=0.047) in addition to lower right ventricular pulmonary artery coupling (end-systolic elastance/arterial elastance 2.24±1.03 versus 1.36±0.37; p=0.006). During the 4-year follow-up period, two unaffected carriers developed pulmonary arterial hypertension, with normal N-terminal pro-brain natriuretic peptide and transthoracic echocardiography indices at diagnosis.
Conclusion: Unaffected BMPR2 mutation carriers have an altered cardiac phenotype mimicked in Bmpr2Δ71Ex1/+ transgenic rats. Future efforts to establish an effective screening protocol for individuals at risk for developing pulmonary arterial hypertension warrant longer follow-up periods.
Copyright ©The authors 2024.
Conflict of interest statement
Conflicts of interest: F. Perros reports grants from French National Research Agency (ANR-20-CE14-0006) and INSERM (International Research Project (IRP) (Paris – Porto Pulmonary Hypertension Collaborative Laboratory (3PH)). D. Montani reports grants from Janssen, MSD and Acceleron; consultation fees from Janssen, MSD, Ferrer and Acceleron; and payment or honoraria for lectures, presentations, manuscript writing or educational events from Bayer, Janssen, Boehringer, Chiesi, GSK, Ferrer and Merck MSD. A. Vonk Nordegraaf reports research grants from Janssen, MSD and Ferrer. L. Zhao reports grants from British Heart Foundation (PG/18/2/33446 and BHF RE/18/4/34215). F.S. de Man reports support for the present study from Royal Netherlands Academy of Sciences (CVON-2017-10 Dolphin-Genesis); grants from Netherlands CardioVascular Research Initiative: the Dutch Heart Foundation, Dutch Federation of University Medical Centres, Netherlands Organisation for Health Research and Development, The Netherlands Organisation for Scientific Research (NWO-VICI: 918.16.610, NWO-VIDI: 917.18.338), Royal Netherlands Academy of Sciences (CVON-2012-08 PHAEDRA and CVON-2018-29 PHAEDRA-IMPACT) and Dutch Heart Foundation (Post doc Dekker 2018T05). H-J. Bogaard reports support for the present study from Royal Netherlands Academy of Sciences (CVON-2017-10 Dolphin-Genesis); grants from MSD, Ferrer, Janssen, Dutch Federation of University Medical Centres, Netherlands CardioVascular Research Initiative: the Dutch Heart Foundation, Netherlands Organisation for Health Research and Development, and the Royal Netherlands Academy of Sciences (CVON-2012-08 PHAEDRA and CVON-2018-29 PHAEDRA-IMPACT). The remaining authors have no potential conflicts of interest to disclose.
Figures
Comment in
-
What to do when pulmonary arterial hypertension screening suggests neither fish nor fowl? The DOLPHIN-GENESIS study.Eur Respir J. 2024 Oct 3;64(4):2401369. doi: 10.1183/13993003.01369-2024. Print 2024 Oct. Eur Respir J. 2024. PMID: 39362685 No abstract available.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous