

Arterial Spin-Labeling MR Imaging in the Detection of Intracranial Arteriovenous Malformations in Patients with Hereditary Hemorrhagic Telangiectasia
- PMID: 38991769
- PMCID: PMC11383423
- DOI: 10.3174/ajnr.A8281
Arterial Spin-Labeling MR Imaging in the Detection of Intracranial Arteriovenous Malformations in Patients with Hereditary Hemorrhagic Telangiectasia
Abstract
Background and purpose: Hereditary hemorrhagic telangiectasia (HHT) is an autosomal dominant disease that causes vascular malformations in a variety of organs and tissues, including brain AVMs. Because brain AVMs have the potential to cause disabling or fatal intracranial hemorrhage, detection of these lesions before rupture is the goal of screening MR imaging/MRA examinations in patients with HHT. Prior studies have demonstrated superior sensitivity for HHT-related brain AVMs by using postcontrast MR imaging sequences as compared with MRA alone. We now present data regarding the incremental benefit of including arterial spin-labeling (ASL) perfusion sequences as part of MR imaging/MRA screening in patients with this condition.
Materials and methods: We retrospectively analyzed 831 patients at the UCSF Hereditary Hemorrhagic Telangiectasia Center of Excellence. Of these, 42 patients had complete MR imaging/MRA, ASL perfusion scans, and criterion-standard DSA data. Two neuroradiologists reviewed imaging studies and a third provided adjudication when needed.
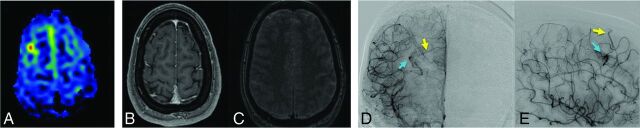
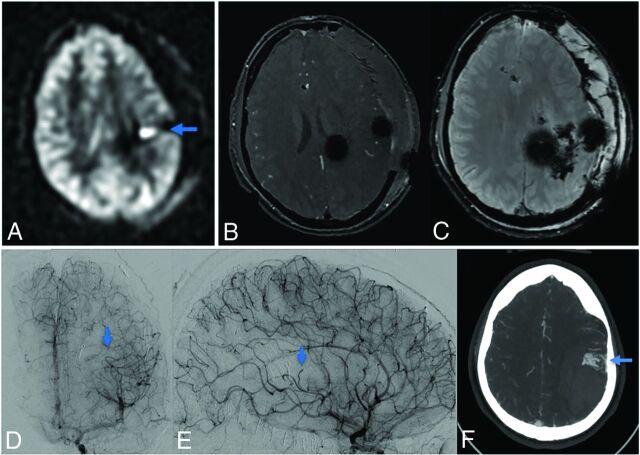
Results: Eight patients had no brain AVMs detected on DSA. The remaining 34 patients had 57 brain AVMs on DSA. Of the 57 identified AVMs, 51 (89.5%) were detected on ASL and 43 (75.4%) were detected on conventional MR imaging/MRA sequences (P = .049), with 8 lesions detected on ASL perfusion but not on conventional MR imaging.
Conclusions: ASL provides increased sensitivity for brain AVMs in patients with HHT. Inclusion of ASL should be considered as part of comprehensive MR imaging/MRA screening protocols for institutions taking care of patients with HHT.
© 2024 by American Journal of Neuroradiology.
Figures
Similar articles
-
Diagnostic Performance of TOF, 4D MRA, Arterial Spin-Labeling, and Susceptibility-Weighted Angiography Sequences in the Post-Radiosurgery Monitoring of Brain AVMs.AJNR Am J Neuroradiol. 2025 Jan 8;46(1):57-65. doi: 10.3174/ajnr.A8420. AJNR Am J Neuroradiol. 2025. PMID: 39025641
-
Current Practice: Rationale for Screening Children with Hereditary Hemorrhagic Telangiectasia for Brain Vascular Malformations.AJNR Am J Neuroradiol. 2024 Sep 9;45(9):1177-1184. doi: 10.3174/ajnr.A8195. AJNR Am J Neuroradiol. 2024. PMID: 38816017 Review.
-
Brain and lung arteriovenous malformation rescreening practices for children and adults with hereditary hemorrhagic telangiectasia.Orphanet J Rare Dis. 2024 Nov 9;19(1):421. doi: 10.1186/s13023-024-03402-8. Orphanet J Rare Dis. 2024. PMID: 39522006 Free PMC article.
-
Computed tomography angiography or magnetic resonance angiography for detection of intracranial vascular malformations in patients with intracerebral haemorrhage.Cochrane Database Syst Rev. 2014 Sep 1;2014(9):CD009372. doi: 10.1002/14651858.CD009372.pub2. Cochrane Database Syst Rev. 2014. PMID: 25177839 Free PMC article.
-
Comparison of MRI, MRA, and DSA for Detection of Cerebral Arteriovenous Malformations in Hereditary Hemorrhagic Telangiectasia.AJNR Am J Neuroradiol. 2020 Jun;41(6):969-975. doi: 10.3174/ajnr.A6549. Epub 2020 May 7. AJNR Am J Neuroradiol. 2020. PMID: 32381546 Free PMC article.
Cited by
-
Hereditary haemorrhagic telangiectasia.Nat Rev Dis Primers. 2025 Jan 9;11(1):1. doi: 10.1038/s41572-024-00585-z. Nat Rev Dis Primers. 2025. PMID: 39788978 Review.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources