

Kidney outcomes with SGLT2 inhibitor versus DPP4 inhibitor use in older adults with diabetes
- PMID: 38991990
- PMCID: PMC11879043
- DOI: 10.1093/ndt/gfae158
Kidney outcomes with SGLT2 inhibitor versus DPP4 inhibitor use in older adults with diabetes
Abstract
Background: While the kidney-protective effects of sodium-glucose co-transporter 2 (SGLT2) inhibitors have attracted much attention, there are limited real-world clinical data examining the effects of SGLT2 inhibitors on kidney function in older individuals. We aimed to compare the kidney outcomes between SGLT2 inhibitor and dipeptidyl peptidase 4 (DPP4) inhibitor use in older adults with diabetes.
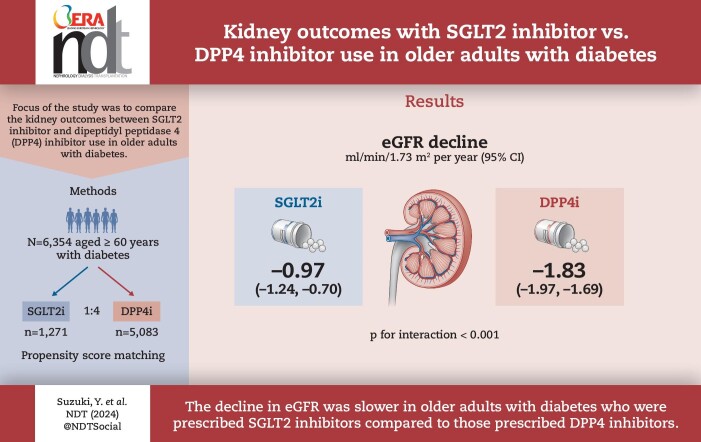
Methods: Using a nationwide claims database, we studied 6354 older adults (≥60 years of age) who had diabetes and were newly initiated on SGLT2 inhibitors or DPP4 inhibitors. A 1:4 propensity score matching algorithm was used to compare changes in estimated glomerular filtration rate (eGFR) between SGLT2 inhibitor and DPP4 inhibitor users. The primary outcome was a decrease in the rate of eGFR, which was obtained using a linear mixed-effects model with an unstructured covariance.
Results: Following propensity score matching, 6354 individuals including 1271 SGLT2 inhibitor users and 5083 DPP4 inhibitor users {median age 68 years [interquartile range (IQR) 65-70], male 60.4%, median eGFR 69.0 ml/min/1.73 m2 [IQR 59.1-79.0], median haemoglobin A1c [HbA1c] 6.9% [IQR 6.5-7.4]} were analysed. SGLT2 inhibitor users had a slower eGFR decline than did DPP4 inhibitor users [-0.97 ml/min/1.73 m2/year (95% CI -1.24 to -0.70) versus -1.83 ml/min/1.73 m2/year (95% CI -1.97 to -1.69); P for interaction <.001]. This finding remained consistent across subgroups based on age, sex, body mass index, HbA1c level, renin-angiotensin system inhibitor use and baseline eGFR. Additionally, the risk of a ≥20%, ≥30% and ≥40% decrease in eGFR from baseline was significantly lower in SGLT2 inhibitor users than in DPP4 inhibitor users.
Conclusions: Our analysis, utilizing a nationwide epidemiological dataset, demonstrated that the decrease in eGFR was slower in individuals ≥60 years of age with diabetes who were prescribed SGLT2 inhibitors compared with those prescribed DPP4 inhibitors, suggesting a potential advantage of SGLT2 inhibitors for kidney outcomes even in older individuals with diabetes.
Keywords: SGLT2 inhibitors; chronic kidney disease; diabetes; epidemiology.
© The Author(s) 2024. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
H.K. and K.F received research funding and scholarship funds from Medtronic Japan, Boston Scientific Japan, Biotronik Japan, Simplex Quantum and Fukuda Denshi. I.K. received remuneration for a lecture from AstraZeneca, MSD, Otsuka Pharmaceutical, Ono Pharmaceutical, Daiichi Sankyo, Mitsubishi Tanabe Pharma, Nippon Boehringer Ingelheim, Bayer Yakuhin, Novo Nordisk Pharma and Pfizer Japan; trust research/joint research funds from Ono Pharmaceutical and scholarship funds from Idorsia Pharmaceuticals Japan, MSD, Ono Pharmaceutical, Sanofi, Daiichi Sankyo, Dainippon Sumitomo Pharma, Takeda Pharmaceutical, Mitsubishi Tanabe Pharma, Teijin Pharma and Toa Eiyo. A.N. received research funding from Bayer Yakuhin, Daiichi Sankyo, Nippon Boehringer Ingelheim and Taisho Pharmaceutical and a participated in speakers bureaus for Daiichi Sankyo, Nippon Boehringer Ingelheim, Novartis Pharma, Mochida Pharmaceutical, AstraZeneca, Mitsubishi Tanabe Pharma and Otsuka Pharmaceutical.
Figures



References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
