

Development and validation of AI-derived segmentation of four-chamber cine cardiac magnetic resonance
- PMID: 38992116
- PMCID: PMC11239622
- DOI: 10.1186/s41747-024-00477-7
Development and validation of AI-derived segmentation of four-chamber cine cardiac magnetic resonance
Abstract
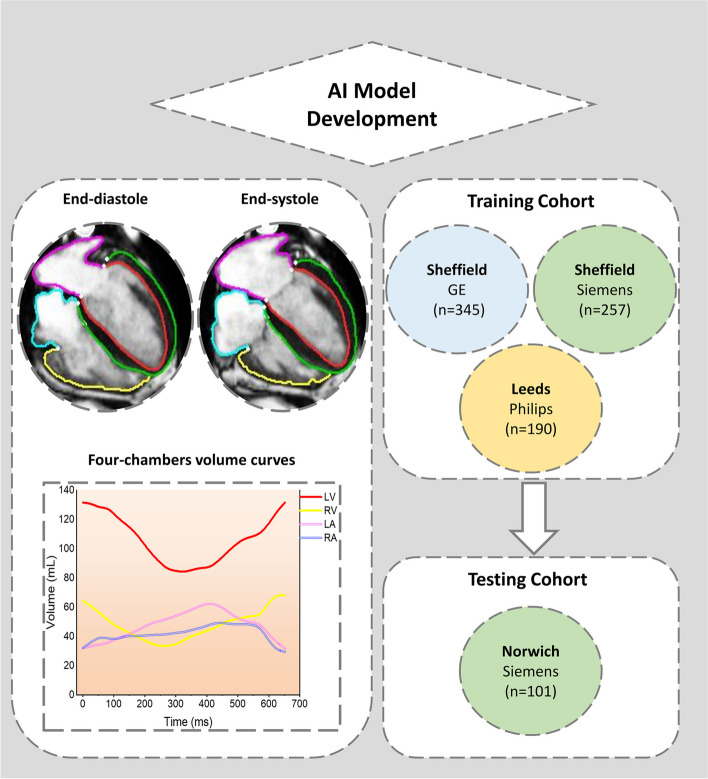
Background: Cardiac magnetic resonance (CMR) in the four-chamber plane offers comprehensive insight into the volumetrics of the heart. We aimed to develop an artificial intelligence (AI) model of time-resolved segmentation using the four-chamber cine.
Methods: A fully automated deep learning algorithm was trained using retrospective multicentre and multivendor data of 814 subjects. Validation, reproducibility, and mortality prediction were evaluated on an independent cohort of 101 subjects.
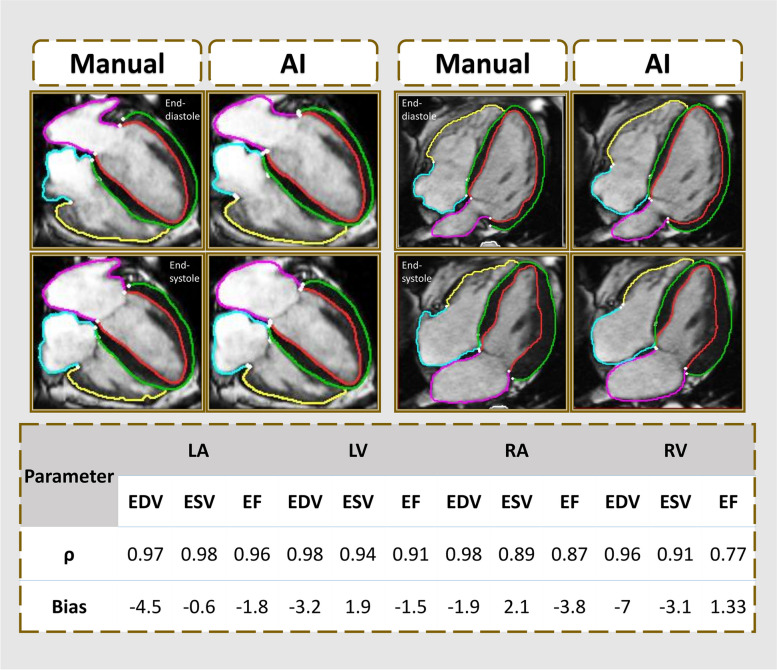
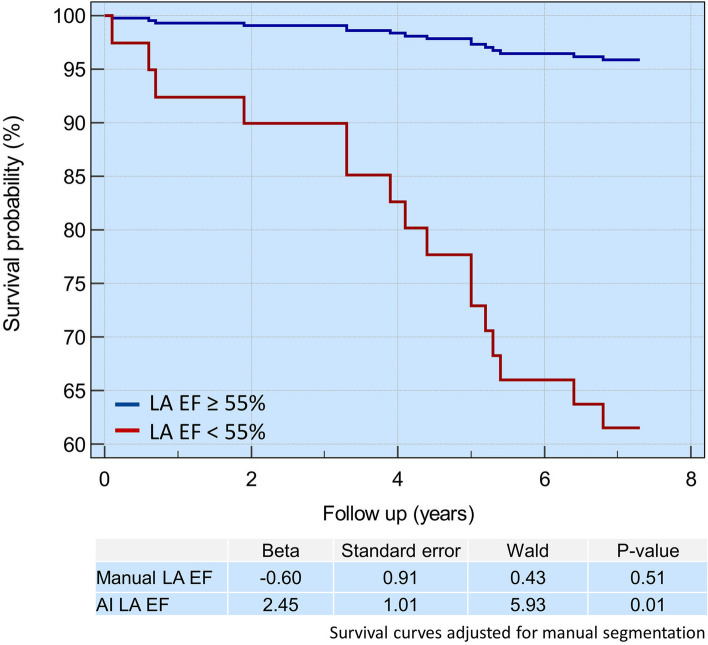
Results: The mean age of the validation cohort was 54 years, and 66 (65%) were males. Left and right heart parameters demonstrated strong correlations between automated and manual analysis, with a ρ of 0.91-0.98 and 0.89-0.98, respectively, with minimal bias. All AI four-chamber volumetrics in repeatability analysis demonstrated high correlation (ρ = 0.99-1.00) and no bias. Automated four-chamber analysis underestimated both left ventricular (LV) and right ventricular (RV) volumes compared to ground-truth short-axis cine analysis. Two correction factors for LV and RV four-chamber analysis were proposed based on systematic bias. After applying the correction factors, a strong correlation and minimal bias for LV volumetrics were observed. During a mean follow-up period of 6.75 years, 16 patients died. On stepwise multivariable analysis, left atrial ejection fraction demonstrated an independent association with death in both manual (hazard ratio (HR) = 0.96, p = 0.003) and AI analyses (HR = 0.96, p < 0.001).
Conclusion: Fully automated four-chamber CMR is feasible, reproducible, and has the same real-world prognostic value as manual analysis. LV volumes by four-chamber segmentation were comparable to short-axis volumetric assessment.
Trials registration: ClinicalTrials.gov: NCT05114785.
Relevance statement: Integrating fully automated AI in CMR promises to revolutionise clinical cardiac assessment, offering efficient, accurate, and prognostically valuable insights for improved patient care and outcomes.
Key points: • Four-chamber cine sequences remain one of the most informative acquisitions in CMR examination. • This deep learning-based, time-resolved, fully automated four-chamber volumetric, functional, and deformation analysis solution. • LV and RV were underestimated by four-chamber analysis compared to ground truth short-axis segmentation. • Correction bias for both LV and RV volumes by four-chamber segmentation, minimises the systematic bias.
Keywords: Artificial intelligence, Deep learning, Heart diseases, Magnetic resonance imaging (cine), Prognosis.
© 2024. The Author(s).
Conflict of interest statement
PG is a clinical advisor for Pie Medical Imaging and Medis Medical Imaging. PG Consults for Anteris Technologies and for Edwards Lifesciences. All other authors have no competing interests to declare.
Figures


Similar articles
-
Assessment of deep learning segmentation for real-time free-breathing cardiac magnetic resonance imaging at rest and under exercise stress.Sci Rep. 2024 Feb 14;14(1):3754. doi: 10.1038/s41598-024-54164-z. Sci Rep. 2024. PMID: 38355969 Free PMC article.
-
Automated cardiovascular magnetic resonance image analysis with fully convolutional networks.J Cardiovasc Magn Reson. 2018 Sep 14;20(1):65. doi: 10.1186/s12968-018-0471-x. J Cardiovasc Magn Reson. 2018. PMID: 30217194 Free PMC article.
-
Automated left and right ventricular chamber segmentation in cardiac magnetic resonance images using dense fully convolutional neural network.Comput Methods Programs Biomed. 2021 Jun;204:106059. doi: 10.1016/j.cmpb.2021.106059. Epub 2021 Mar 21. Comput Methods Programs Biomed. 2021. PMID: 33812305
-
Artificial intelligence for left ventricular hypertrophy detection and differentiation on echocardiography, cardiac magnetic resonance and cardiac computed tomography: A systematic review.Int J Cardiol. 2025 Mar 1;422:132979. doi: 10.1016/j.ijcard.2025.132979. Epub 2025 Jan 10. Int J Cardiol. 2025. PMID: 39798885
-
A review of heart chamber segmentation for structural and functional analysis using cardiac magnetic resonance imaging.MAGMA. 2016 Apr;29(2):155-95. doi: 10.1007/s10334-015-0521-4. Epub 2016 Jan 25. MAGMA. 2016. PMID: 26811173 Free PMC article. Review.
Cited by
-
Artificial Intelligence in Cardiovascular Imaging: Current Landscape, Clinical Impact, and Future Directions.Discoveries (Craiova). 2025 Jun 30;13(1):e211. doi: 10.15190/d.2025.10. eCollection 2025 Apr-Jun. Discoveries (Craiova). 2025. PMID: 40771296 Free PMC article. Review.
-
Artificial Intelligence Performance in Cardiac Magnetic Resonance Strain Analysis for Aortic Stenosis: Validation with Echocardiography and Healthy Controls.Medicina (Kaunas). 2025 May 22;61(6):950. doi: 10.3390/medicina61060950. Medicina (Kaunas). 2025. PMID: 40572638 Free PMC article.
-
Automated Quantification of Simple and Complex Aortic Flow Using 2D Phase Contrast MRI.Medicina (Kaunas). 2024 Oct 3;60(10):1618. doi: 10.3390/medicina60101618. Medicina (Kaunas). 2024. PMID: 39459405 Free PMC article.
-
Curriculum check, 2025-equipping radiology residents for AI challenges of tomorrow.Abdom Radiol (NY). 2025 Jun 9. doi: 10.1007/s00261-025-05016-5. Online ahead of print. Abdom Radiol (NY). 2025. PMID: 40488865 Review.
-
Segmentation-Free Estimation of Left Ventricular Ejection Fraction Using 3D CNN Is Reliable and Improves as Multiple Cardiac MRI Cine Orientations Are Combined.Biomedicines. 2024 Oct 12;12(10):2324. doi: 10.3390/biomedicines12102324. Biomedicines. 2024. PMID: 39457634 Free PMC article.
References
-
- Alabed S, Maiter A, Mahmood A, et al. Quality of reporting of artificial intelligence studies: Lessons learnt from a systematic review of the literature. Clin Radiol. 2022;77:e21. doi: 10.1016/J.CRAD.2022.09.057. - DOI
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical