

Fluid management for sepsis-induced hypotension in patients with advanced chronic kidney disease: a secondary analysis of the CLOVERS trial
- PMID: 38992663
- PMCID: PMC11238412
- DOI: 10.1186/s13054-024-05019-6
Fluid management for sepsis-induced hypotension in patients with advanced chronic kidney disease: a secondary analysis of the CLOVERS trial
Abstract
Background: Early fluid management in patients with advanced chronic kidney disease (CKD) and sepsis-induced hypotension is challenging with limited evidence to support treatment recommendations. We aimed to compare an early restrictive versus liberal fluid management for sepsis-induced hypotension in patients with advanced CKD.
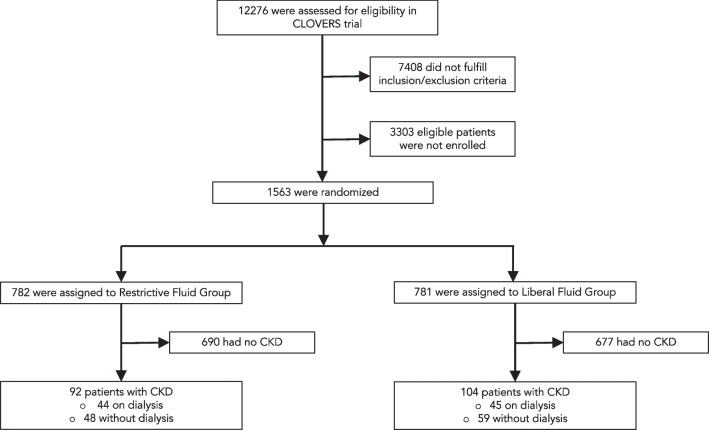
Methods: This post-hoc analysis included patients with advanced CKD (eGFR of less than 30 mL/min/1.73 m2 or history of end-stage renal disease on chronic dialysis) from the crystalloid liberal or vasopressor early resuscitation in sepsis (CLOVERS) trial. The primary endpoint was death from any cause before discharge home by day 90.
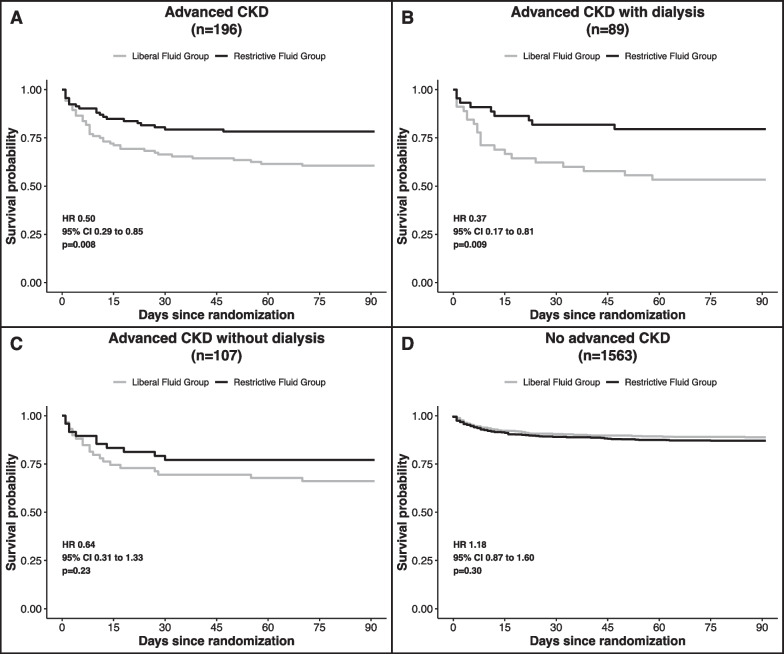
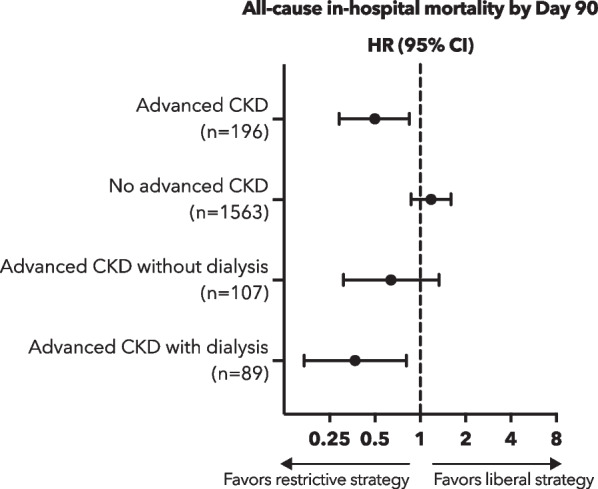
Results: Of 1563 participants enrolled in the CLOVERS trial, 196 participants had advanced CKD (45% on chronic dialysis), with 92 participants randomly assigned to the restrictive treatment group and 104 assigned to the liberal fluid group. Death from any cause before discharge home by day 90 occurred significantly less often in the restrictive fluid group compared with the liberal fluid group (20 [21.7%] vs. 41 [39.4%], HR 0.5, 95% CI 0.29-0.85). Participants in the restrictive fluid group had more vasopressor-free days (19.7 ± 10.4 days vs. 15.4 ± 12.6 days; mean difference 4.3 days, 95% CI, 1.0-7.5) and ventilator-free days by day 28 (21.0 ± 11.8 vs. 16.5 ± 13.6 days; mean difference 4.5 days, 95% CI, 0.9-8.1).
Conclusions: In patients with advanced CKD and sepsis-induced hypotension, an early restrictive fluid strategy, prioritizing vasopressor use, was associated with a lower risk of death from any cause before discharge home by day 90 as compared with an early liberal fluid strategy.
Trial registration: NCT03434028 (2018-02-09), BioLINCC 14149.
Keywords: Bacteremia; Chronic kidney disease; Dialysis; Hypervolemia; Septic shock; Vasopressor.
© 2024. The Author(s).
Conflict of interest statement
No author reports conflict of interests relevant to this work.
Figures

References
-
- Malbrain M, Van Regenmortel N, Saugel B, De Tavernier B, Van Gaal PJ, Joannes-Boyau O, et al. Principles of fluid management and stewardship in septic shock: it is time to consider the four D's and the four phases of fluid therapy. Ann Intensive Care. 2018;8(1):66. doi: 10.1186/s13613-018-0402-x. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
