

Staphylococcus aureus screening and preoperative decolonisation with Mupirocin and Chlorhexidine to reduce the risk of surgical site infections in orthopaedic surgery: a pre-post study
- PMID: 38992708
- PMCID: PMC11238515
- DOI: 10.1186/s13756-024-01432-2
Staphylococcus aureus screening and preoperative decolonisation with Mupirocin and Chlorhexidine to reduce the risk of surgical site infections in orthopaedic surgery: a pre-post study
Abstract
Background: Nasal carriage of Staphylococcus aureus is a risk factor for surgical site infections (SSI) in orthopaedic surgery. The efficacy of decolonisation for S. aureus on reducing the risk of SSI is uncertain in this speciality. The objective was to evaluate the impact of a nasal screening strategy of S. aureus and targeted decolonisation on the risk of S. aureus SSI.
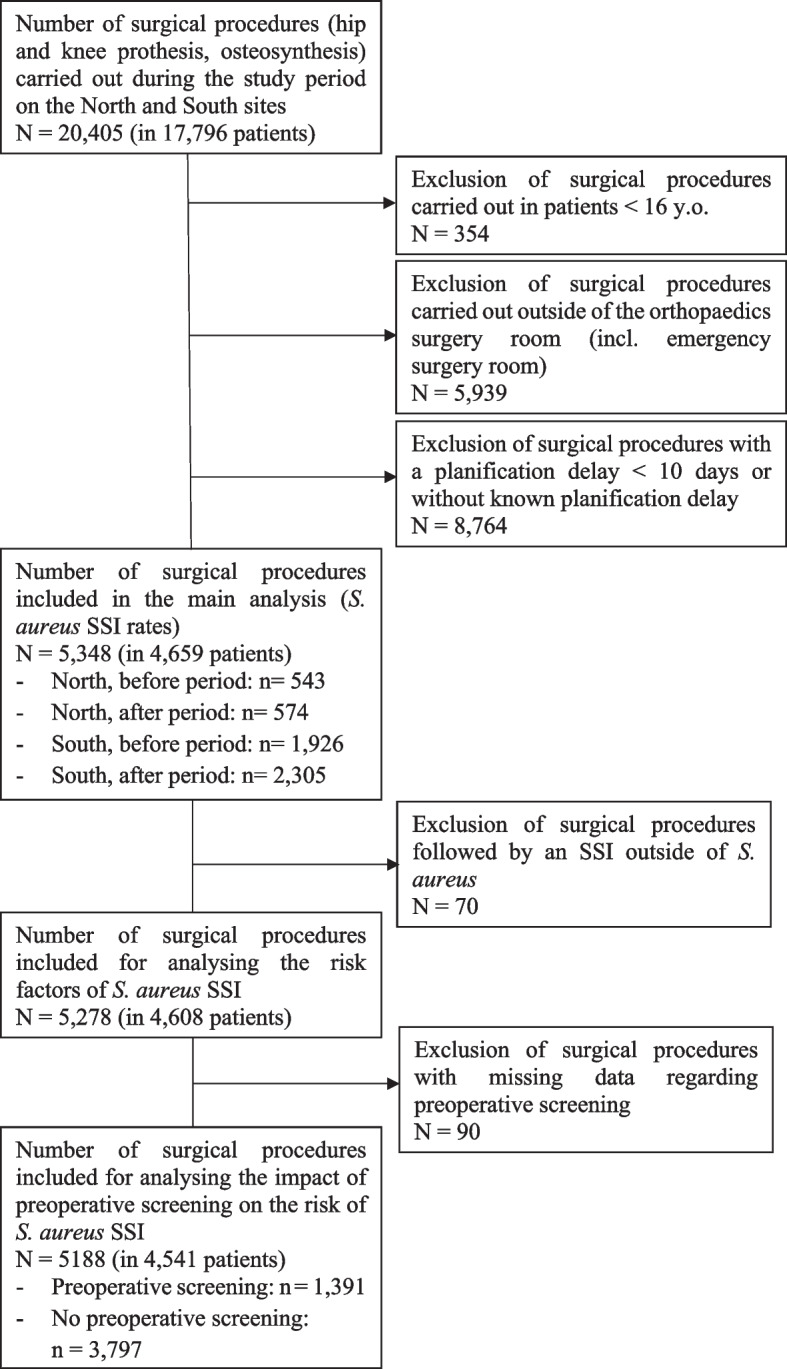
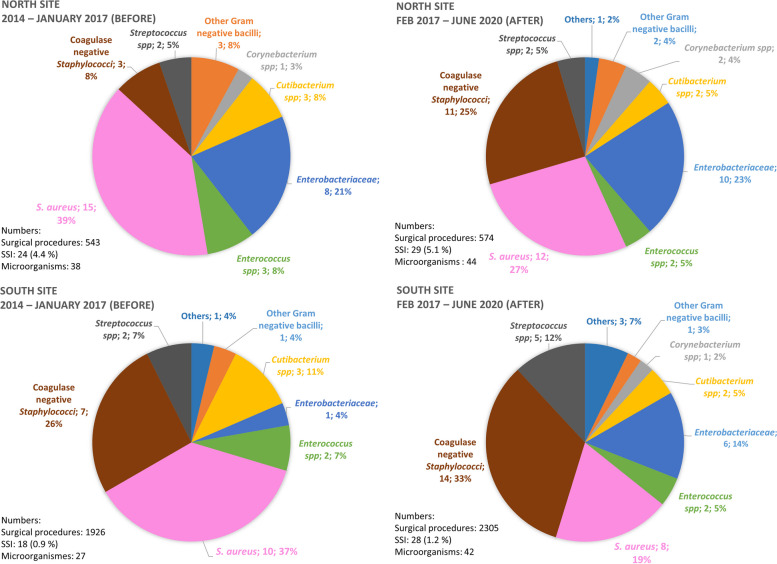
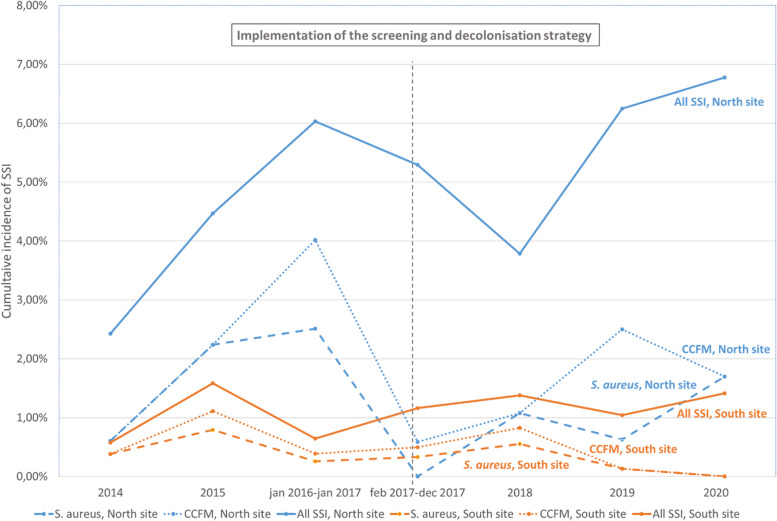
Methods: A retrospective pre-post and here-elsewhere study was conducted between January 2014 and June 2020 in 2 adult orthopaedic surgical sites (North and South) of a French university hospital. Decolonisation with Mupirocin and Chlorhexidine was conducted in S. aureus carriers starting February 2017 in the South site (intervention group). Scheduled surgical procedures for hip, knee arthroplasties, and osteosyntheses were included and monitored for one year. The rates of S. aureus SSI in the intervention group were compared to a historical control group (South site) and a North control group. The risk factors for S. aureus SSI were analysed by logistic regression.
Results: A total of 5,348 surgical procedures was included, 100 SSI of which 30 monomicrobial S. aureus SSI were identified. The preoperative screening result was available for 60% (1,382/2,305) of the intervention group patients. Among these screenings, 25.3% (349/1,382) were positive for S. aureus and the efficacy of the decolonisation was 91.6% (98/107). The rate of S. aureus SSI in the intervention group (0.3%, 7/2,305) was not significantly different from the historical control group (0.5%, 9/1926) but differed significantly from the North control group (1.3%, 14/1,117). After adjustment, the risk factors of S. aureus SSI occurrence were the body mass index (ORaper unit, 1.05; 95%CI, 1.0-1.1), the Charlson comorbidity index (ORaper point, 1.34; 95%CI, 1.0-1.8) and operative time (ORaper minute, 1.01; 95%CI, 1.00-1.02). Having benefited from S. aureus screening/decolonisation was a protective factor (ORa, 0.24; 95%CI, 0.08-0.73).
Conclusions: Despite the low number of SSI, nasal screening and targeted decolonisation of S. aureus were associated with a reduction in S. aureus SSI.
Keywords: Staphylococcus aureus; Chlorhexidine; Decolonisation; Mupirocin; Screening; Surgical site infection.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Surveillance des infections du site opératoire dans les établissements de santé français. Mission Spicmi, septembre 2020, données 2018 du réseau ISO Raisin. Santé publique France, 2020. https://www.santepubliquefrance.fr/content/download/373269/3152059?versi.... Accessed 6 Feb 2024.
-
- Levy PY, Ollivier M, Drancourt M, Raoult D, Argenson JN. Relation between nasal carriage of Staphylococcus aureus and surgical site infection in orthopedic surgery: The role of nasal contamination. A systematic literature review and meta-analysis. Orthop Traumatol Surg Res. 2013;99:645–51. doi: 10.1016/j.otsr.2013.03.030. - DOI - PubMed
-
- Nakamura M, Shimakawa T, Nakano S, Chikawa T, Yoshioka S, Kashima M, et al. Screening for nasal carriage of Staphylococcus aureus among patients scheduled to undergo orthopedic surgery: Incidence of surgical site infection by nasal carriage. J Orthop Sci. 2017;22:778–82. doi: 10.1016/j.jos.2017.03.005. - DOI - PubMed
-
- Global guidelines for the prevention of surgical site infection [Internet]. 2nd ed. World Health Organization, 2018. https://apps.who.int/iris/handle/10665/277399. Accessed 6 Feb 2024. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
