

Comparison of Outcomes Between Partial and Radical Laparoscopic Nephrectomy for Localized Renal Tumors Larger Than Four Centimeters: A Systematic Review and Meta-Analysis
- PMID: 38993256
- PMCID: PMC11236382
- DOI: 10.14740/wjon1866
Comparison of Outcomes Between Partial and Radical Laparoscopic Nephrectomy for Localized Renal Tumors Larger Than Four Centimeters: A Systematic Review and Meta-Analysis
Abstract
Background: Earlier studies have juxtaposed different laparoscopic methods for treating renal tumors; however, extensive evidence with a particular focus on large kidney tumors remains lacking. The objective of this meta-analysis was to assess the perioperative outcomes, kidney performance, and cancer-related results of laparoscopic partial nephrectomy (LPN) versus laparoscopic radical nephrectomy (LRN) for treating extensive, localized, non-metastatic kidney tumors (cT1b-cT2N0M0).
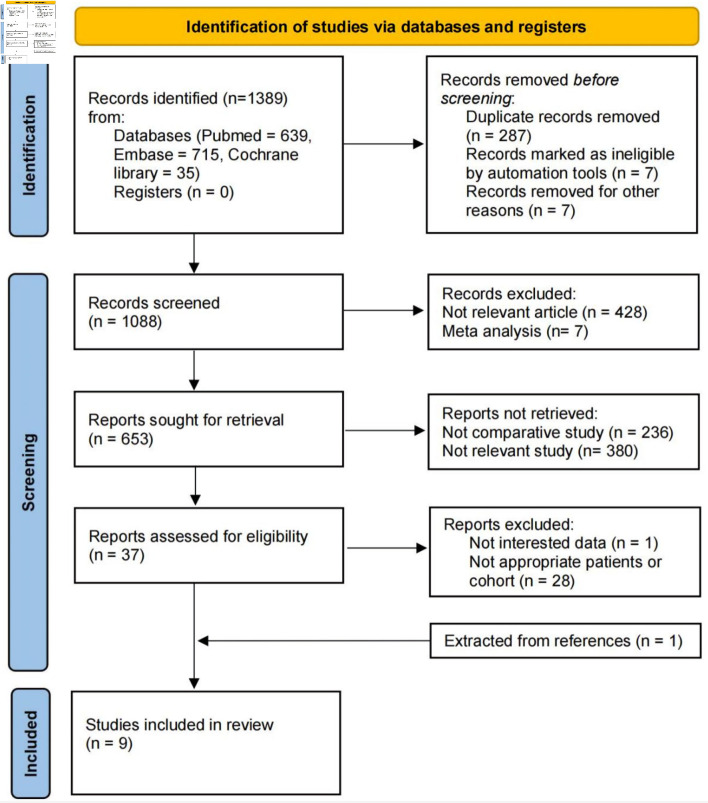
Methods: We systematically searched multiple databases from database inception until December 2023 for relevant studies. Selected data were analyzed with the Cochrane Collaboration's Review Manager 5.4 software using a random-effects model. Outcomes were expressed as odds ratios and weighted mean differences with 95% confidence intervals, considering a P value of < 0.05 as significant.
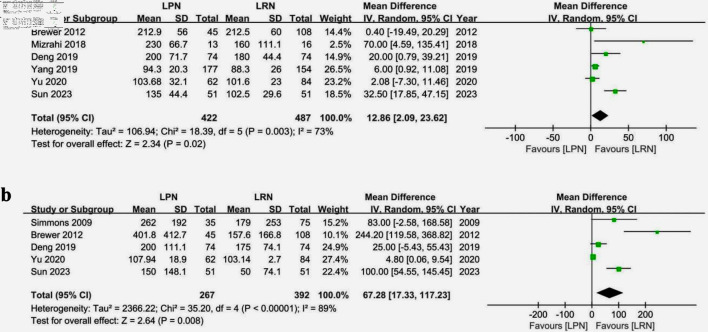
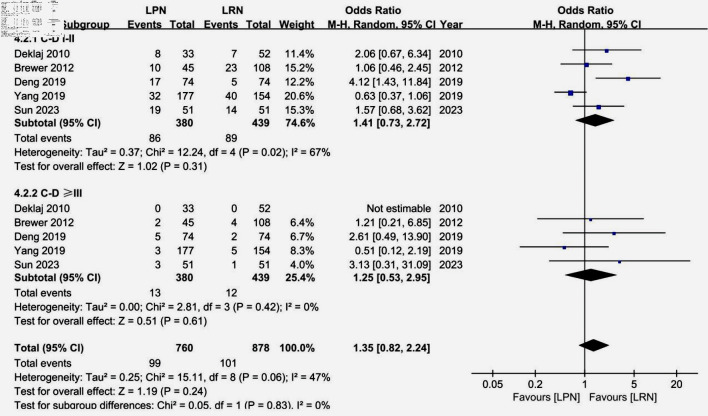
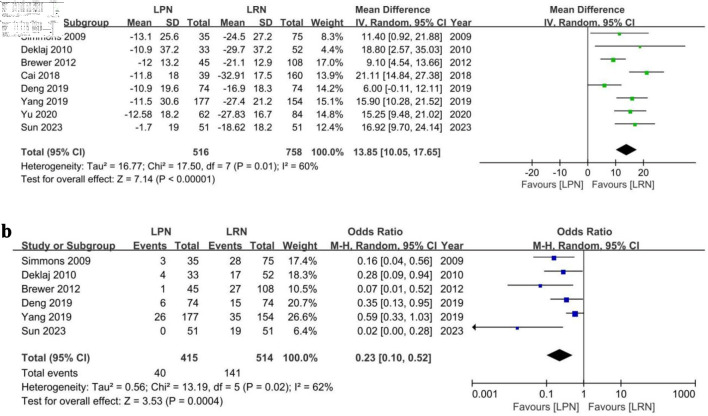
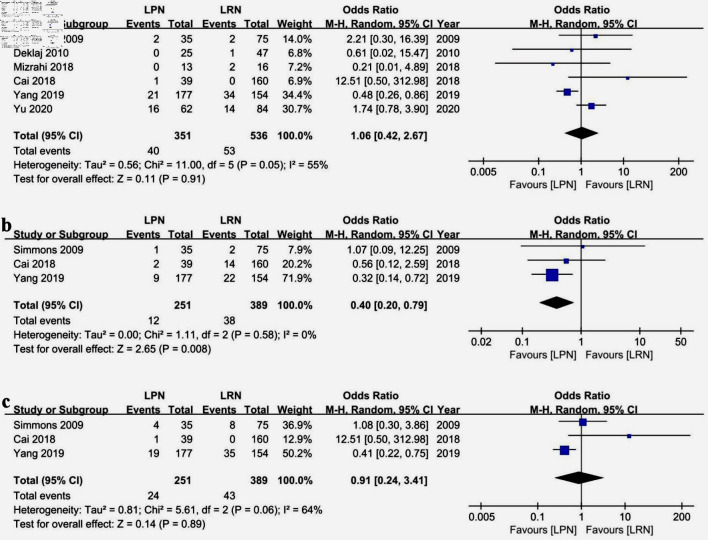
Results: Data from nine studies encompassing 1,303 patients (529 LPN, 774 LRN) revealed that LPN was associated with lengthier surgeries and increased blood loss compared to LRN. While LPN exhibited higher postoperative complication rates, the disparity did not reach statistical significance. LPN led to improved postoperative renal function, manifesting as a reduced estimated glomerular filtration rate (eGFR) decline and fewer incidents of new chronic kidney disease cases. Both groups demonstrated comparable tumor recurrence and overall mortality rates, but LPN exhibited significantly lower cancer-specific mortality rates.
Conclusions: LPN, despite longer operative times and greater intraoperative blood loss, was found to be superior to LRN in preserving postoperative renal function. Oncologically, LPN and LRN have comparable overall mortality rates, but LPN showed a significant advantage in terms of lower cancer-specific mortality rates.
Keywords: Kidney neoplasms; Laparoscopy; Meta-analysis; Nephrectomy; Systematic review.
Copyright 2024, Dong et al.
Conflict of interest statement
All authors have no conflict of interest to disclose.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous