

Adrenal Mass and Hypokalaemia: The Zebra Among Horses
- PMID: 38993410
- PMCID: PMC11237954
- DOI: 10.7759/cureus.62123
Adrenal Mass and Hypokalaemia: The Zebra Among Horses
Abstract
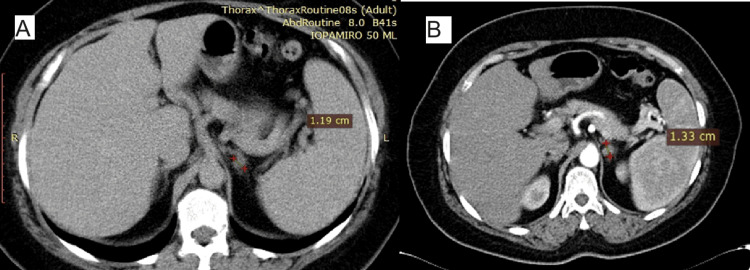
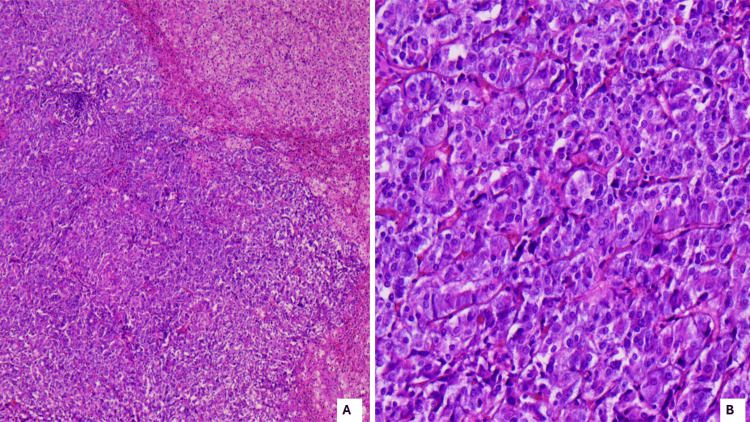
Pheochromocytoma rarely presents with unexplained hypokalaemia, although there are some case reports in the literature. The mechanism behind this could be the increased cellular potassium uptake promoted by beta-2-adrenoreceptor hyperactivation and insulin resistance. We present the case of a 68-year-old hypertensive female patient with a unilateral adrenal mass discovered on angio-CT and typical signs of adrenergic hyperstimulation (hypertensive crisis, headache, and sweating) associated with multiple arrhythmic episodes but with normal plasma and urinary catecholamine levels. During the work-up for hormonal hypersecretion and the cessation of anti-aldosterone medication, the patient presented resistant hypokalaemia. Due to uncorrectable hypokalaemia, we were unable to perform hormonal investigations for primary hyperaldosteronism and referred the patient for laparoscopic adrenalectomy. The histological diagnosis revealed left pheochromocytoma. Postoperatively, the patient experienced rebound hyperkalaemia. In a patient with a unilateral adrenal mass and hypokalaemia, besides primary hyperaldosteronism and adrenocorticotropic hormone-independent hypercortisolism, a possible pheochromocytoma should be ruled out as well by the clinician before surgery.
Keywords: adrenal mass; electrolyte imbalance; hypertension; hypokalaemia; pheochromocytoma.
Copyright © 2024, Reti et al.
Conflict of interest statement
Human subjects: Consent was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Pitfalls in the diagnosis and treatment of a hypertensive patient with unilateral primary aldosteronism and contralateral pheochromocytoma: a case report.BMC Endocr Disord. 2023 Feb 16;23(1):44. doi: 10.1186/s12902-023-01297-3. BMC Endocr Disord. 2023. PMID: 36797699 Free PMC article.
-
Catastrophic ACTH-secreting pheochromocytoma: an uncommon and challenging entity with multifaceted presentation.Endocrinol Diabetes Metab Case Rep. 2023 May 2;2023(2):22-0308. doi: 10.1530/EDM-22-0308. Print 2023 May 1. Endocrinol Diabetes Metab Case Rep. 2023. PMID: 37162230 Free PMC article.
-
Review of surgical management of aldosterone secreting tumours of the adrenal cortex.Eur J Surg Oncol. 2003 Jun;29(5):467-74. doi: 10.1016/s0748-7983(03)00051-9. Eur J Surg Oncol. 2003. PMID: 12798753
-
Aldosterone-secreting adrenal cortical adenoma in an 11-year-old child and collective review of the literature.Eur J Pediatr. 1994 Oct;153(10):715-7. doi: 10.1007/BF01954485. Eur J Pediatr. 1994. PMID: 7813526 Review.
-
Aldosterone-secreting adrenal cortical adenoma in an 11-year-old child and collective review of the literature.Eur J Pediatr. 1994 Jul;153(7):480-2. doi: 10.1007/BF01957000. Eur J Pediatr. 1994. PMID: 7957362 Review.
References
-
- European Society of Endocrinology clinical practice guidelines on the management of adrenal incidentalomas, in collaboration with the European Network for the Study of Adrenal Tumors. Fassnacht M, Tsagarakis S, Terzolo M, et al. https://doi.org/10.1093/ejendo/lvad066 Eur J Endocrinol. 2023;189:0. - PubMed
-
- The management of primary aldosteronism: case detection, diagnosis, and treatment: an Endocrine Society Clinical Practice Guideline. Funder JW, Carey RM, Mantero F, et al. J Clin Endocrinol Metab. 2016;101:1889–1916. - PubMed
-
- A simplified diagnostic approach to pheochromocytoma. A review of the literature and report of one institution's experience. Stein PP, Black HR. Medicine (Baltimore) 1991;70:46–66. - PubMed
-
- Hypokalemia in a patient with pheochromocytoma. Molison MS, Barbagallo J, Mohapatra C, Streeten DH, Numann PJ. Endocr Pract. 1996;2:326–329. - PubMed
-
- Phaeochromocytoma: a case study. Foggo J. Clinical Chiropractic. 2003;6:50–54.
Publication types
LinkOut - more resources
Full Text Sources