

A Case of Endoscopic Partial Transverse Process and Sacral Alar Resection for Bertolotti's Syndrome and Continued Basketball Playing Two Years After Surgery
- PMID: 38993412
- PMCID: PMC11238889
- DOI: 10.7759/cureus.62182
A Case of Endoscopic Partial Transverse Process and Sacral Alar Resection for Bertolotti's Syndrome and Continued Basketball Playing Two Years After Surgery
Abstract
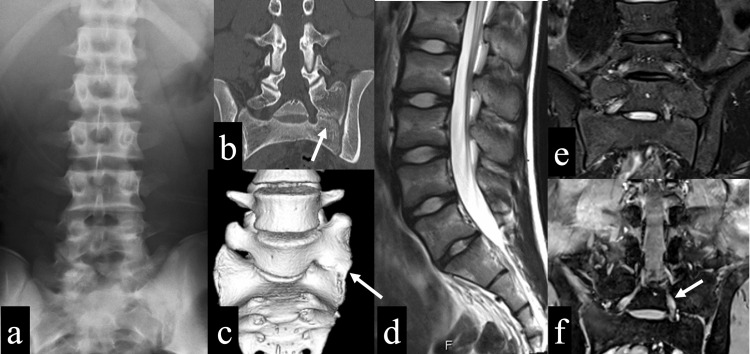
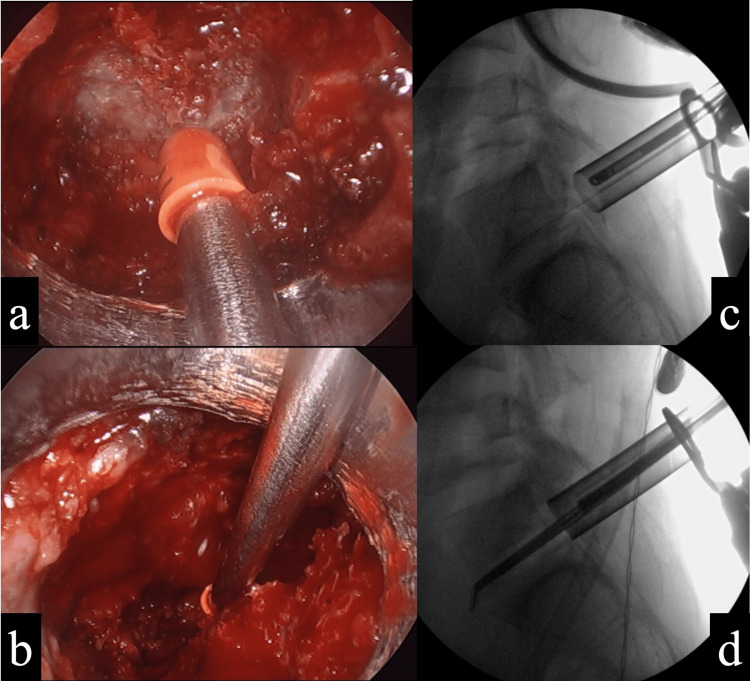
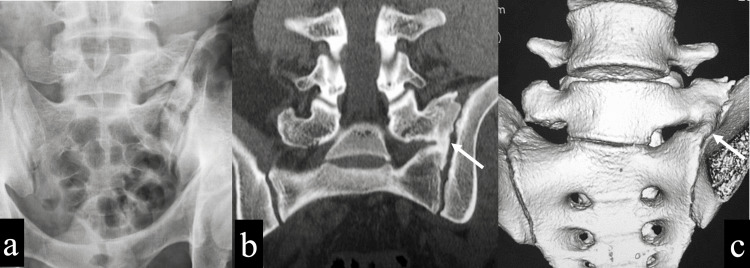
Bertolotti's syndrome is a syndrome in which the transverse process of the most caudal lumbar vertebra becomes enlarged and articulates with the sacral alar, causing back pain. Here, we report a case of an adolescent basketball player with Bertolotti's syndrome who was unable to resume playing despite conservative treatment and underwent an endoscopic partial transverse process and sacral alar resection. A 16-year-old male basketball player presented to our hospital with a chief complaint of left low back pain during exercise and prolonged sitting for over one month. No obvious neurological abnormality was found. X-rays and CT showed lumbosacral transitional vertebrae, and the left transverse process of the sixth lumbar vertebra articulated with the sacrum and iliac, which was the Castellvi classification IIA. A block injection into the articulated surface produced improvement in pain, but the effect was not sustained. Since the patient was refractory to conservative treatments, such as medication and physiotherapy, surgery was performed. During surgery, the articulated transverse process and sacral alar were partially resected endoscopically. Because of the proximity of the resection site to the S1 nerve root, intraoperative electromyography (free-run EMG) was used to detect nerve root irritation symptoms in real time. The patient had no postoperative complications, his low back pain improved immediately, and he returned to play basketball three months after surgery. One year after surgery, the bone resection site showed gradual bone regeneration, and two years after surgery, the transverse process and sacral alar showed a bony bridge. The transverse process was enlarged compared to immediately after surgery but remained smaller than that before surgery. The patient continued to play basketball for two years after surgery without back pain, and no symptoms due to bone regeneration appeared. In the present case, a partial resection of the transverse process and sacral alar was performed with good results. Because the bone resection site was close to the S1 nerve root, the use of an endoscope and intraoperative free-run EMG allowed for a safer procedure during the bone resection. In addition, the patient did not present with symptoms that would affect his basketball performance, although the bone regenerated and bridging occurred between the transverse process and sacral alar over a two-year postoperative course.
Keywords: articulation of the transverse process with the sacral alar and iliac crest; basketball; bertolotti’s syndrome; bone regeneration; bone resection; castellvi classification iia; endoscopic surgery; intraoperative electromyography; low back pain; minimum invasive surgery.
Copyright © 2024, Tatsumura et al.
Conflict of interest statement
Human subjects: Consent was obtained or waived by all participants in this study. Review Board of Tsukuba University Hospital Mito Clinical Education and Training Center/Mito Kyodo General Hospital issued approval 24-07. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures



Similar articles
-
Intraoperative navigation-guided resection of anomalous transverse processes in patients with Bertolotti's syndrome.Surg Neurol Int. 2017 Sep 26;8:236. doi: 10.4103/sni.sni_173_17. eCollection 2017. Surg Neurol Int. 2017. PMID: 29026672 Free PMC article.
-
Decompressive L5 Transverse Processectomy for Bertolotti's Syndrome: A Preliminary Study.Pain Physician. 2017 Sep;20(6):E923-E932. Pain Physician. 2017. PMID: 28934796
-
Surgical Treatment of a Rare Presentation of Bertolotti's Syndrome from Castellvi Type IV Lumbosacral Transitional Vertebra: Case Report and Review of the Literature.J Neurol Surg Rep. 2018 Jul;79(3):e70-e74. doi: 10.1055/s-0038-1667172. Epub 2018 Jul 30. J Neurol Surg Rep. 2018. PMID: 30083494 Free PMC article.
-
Transitional lumbosacral vertebrae and low back pain: diagnostic pitfalls and management of Bertolotti's syndrome.Arq Neuropsiquiatr. 2009 Jun;67(2A):268-72. doi: 10.1590/s0004-282x2009000200018. Arq Neuropsiquiatr. 2009. PMID: 19547821 Review.
-
A systematic review and bibliometric study of Bertolotti's syndrome: clinical characteristics and global trends.Int J Surg. 2023 Oct 1;109(10):3159-3168. doi: 10.1097/JS9.0000000000000541. Int J Surg. 2023. PMID: 37318877 Free PMC article.
References
-
- Back pain in young athletes. Significant differences from adults in causes and patterns. Micheli LJ, Wood R. Arch Pediatr Adolesc Med. 1995;149:15–18. - PubMed
-
- Lumbosacral transitional vertebrae and their relationship with lumbar extradural defects. Castellvi AE, Goldstein LA, Chan DP. Spine (Phila Pa 1976) 1984;9:493–495. - PubMed
Publication types
LinkOut - more resources
Full Text Sources