

Upper Gastrointestinal (GI) Manifestations of Inflammatory Myositis: A Tale of Two Patients
- PMID: 38993454
- PMCID: PMC11238612
- DOI: 10.7759/cureus.62153
Upper Gastrointestinal (GI) Manifestations of Inflammatory Myositis: A Tale of Two Patients
Abstract
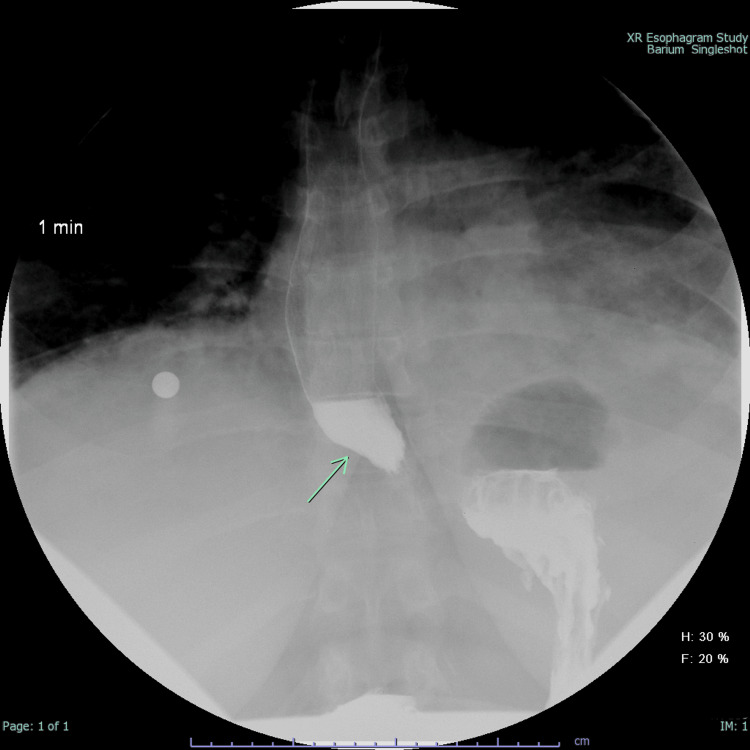
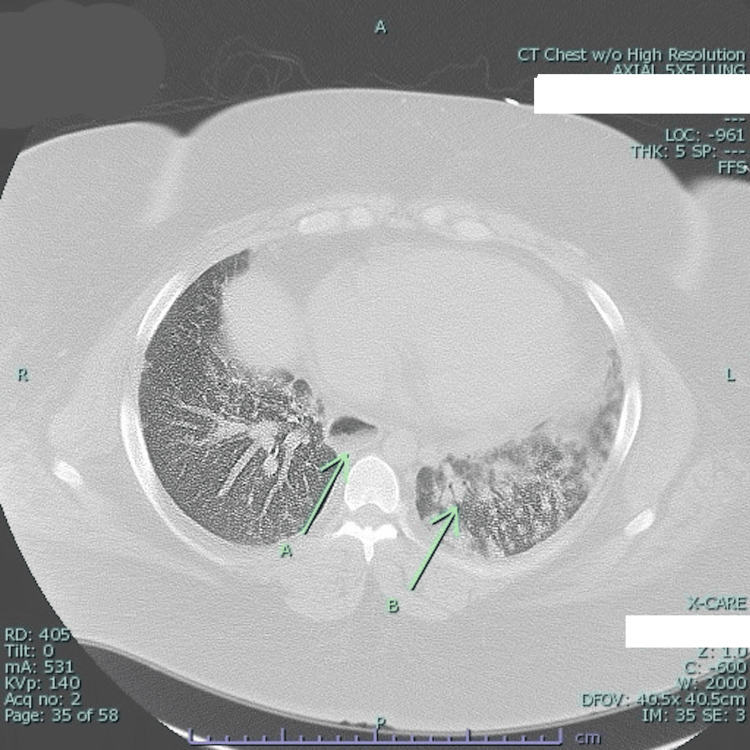
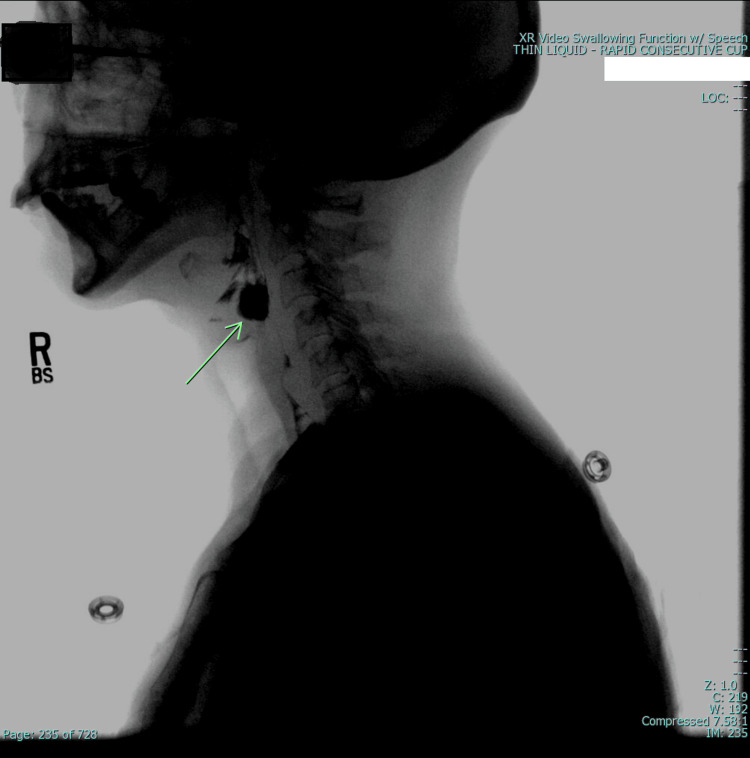
Myositis is a group of rare autoimmune disorders characterized by chronic inflammation of skeletal muscles that leads to a hallmark triad of muscle weakness, fatigue, and myalgia. Extra-muscular manifestations are sometimes seen and involve various organ systems, including the gastrointestinal (GI) tract. In this case series, two patients with polymyositis (PM) and dermatomyositis (DM), both of whom developed dysphagia as a complication of myositis, are discussed. Case 1 was a female with a known history of biopsy-proven dermatomyositis who presented with progressive peripheral edema and weakness affecting all extremities. Concurrently, she displayed symptoms of pneumonia and dysphagia associated with frequent spontaneous or self-induced vomiting to alleviate retrosternal discomfort. Esophagogastroduodenoscopy (EGD) revealed esophageal dilatation and an absence of a contractile response, consistent with myositis. Treatment comprised intravenous immunoglobulin (IVIG), mycophenolate, and lifestyle modifications, including dietary adjustments and maintaining an upright position postprandial. The second case was a female with muscle weakness and dysphagia. Video-fluoroscopic swallow assessment was significant for pharyngeal dysfunction without a sensory response to penetrated material, and the patient was at high risk of aspiration with any oral intake. The presence of pharyngeal dysfunction and dysphagia prompted treatment with IVIG, mycophenolate, and percutaneous endoscopic gastrostomy (PEG) tube placement. These cases have highlighted the upper GI complications observed in patients with myositis, accentuating the necessity for a personalized treatment approach. Timely intervention has shown promising results in symptomatic relief and improving patient outcomes. This emphasizes the importance of a multidisciplinary approach when addressing myositis-related upper GI manifestations.
Keywords: academic rheumatology; intravenous immunoglobulins (ivig); oropharyngeal dysphagia; polymyositis myalgia; s: dermatomyositis.
Copyright © 2024, Hakobyan et al.
Conflict of interest statement
Human subjects: Consent was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Classification and management of adult inflammatory myopathies. Selva-O'Callaghan A, Pinal-Fernandez I, Trallero-Araguás E, Milisenda JC, Grau-Junyent JM, Mammen AL. https://pubmed.ncbi.nlm.nih.gov/30129477/ Lancet Neurol. 2018;17:816–828. - PMC - PubMed
-
- Dysphagia in myositis: a study of the structural and physiologic changes resulting in disordered swallowing. Azola A, Mulheren R, Mckeon G, Lloyd T, Christopher-Stine L, Palmer J, Chung TH. Am J Phys Med Rehabil. 2020;99:404–408. - PubMed
-
- Intravenous immunoglobulin in idiopathic inflammatory myopathies: a practical guide for clinical use. Gandiga PC, Ghetie D, Anderson E, Aggrawal R. Curr Rheumatol Rep. 2023;25:152–168. - PubMed
Publication types
LinkOut - more resources
Full Text Sources