

Optimizing the detection of emerging infections using mobility-based spatial sampling
- PMID: 38993519
- PMCID: PMC11234252
- DOI: 10.1016/j.jag.2024.103949
Optimizing the detection of emerging infections using mobility-based spatial sampling
Abstract
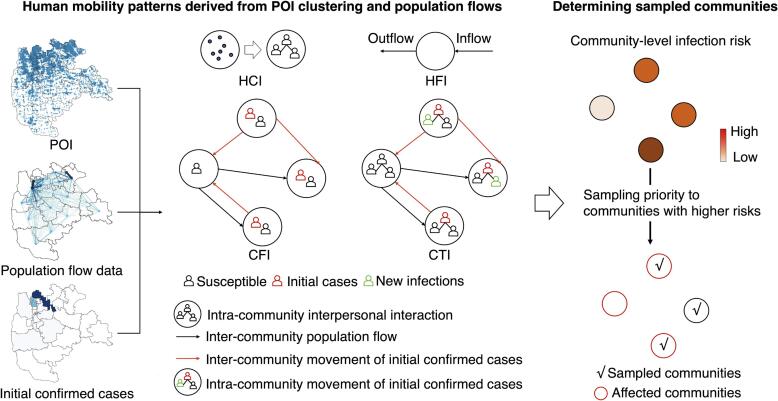
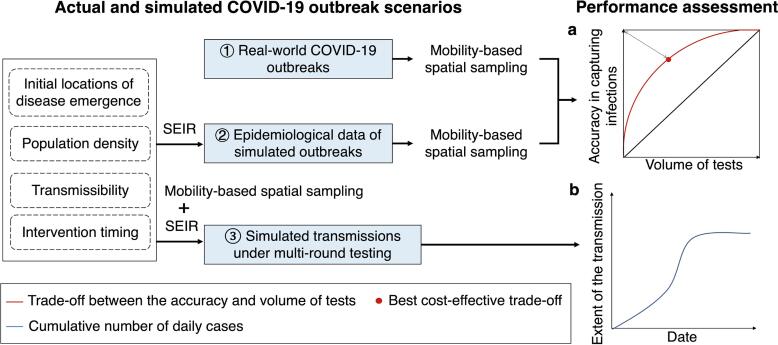
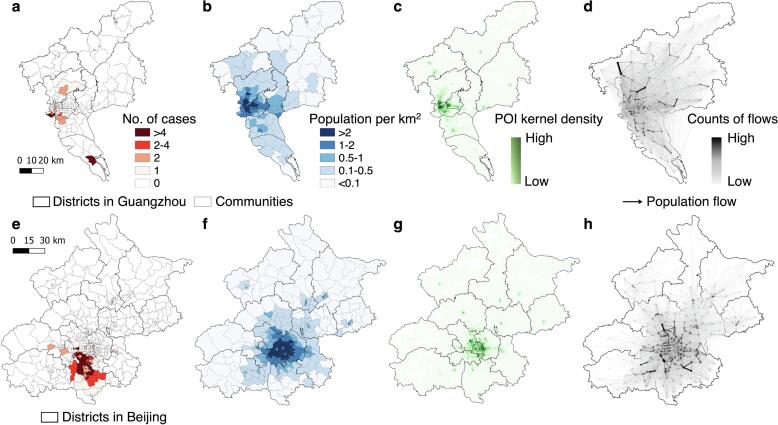
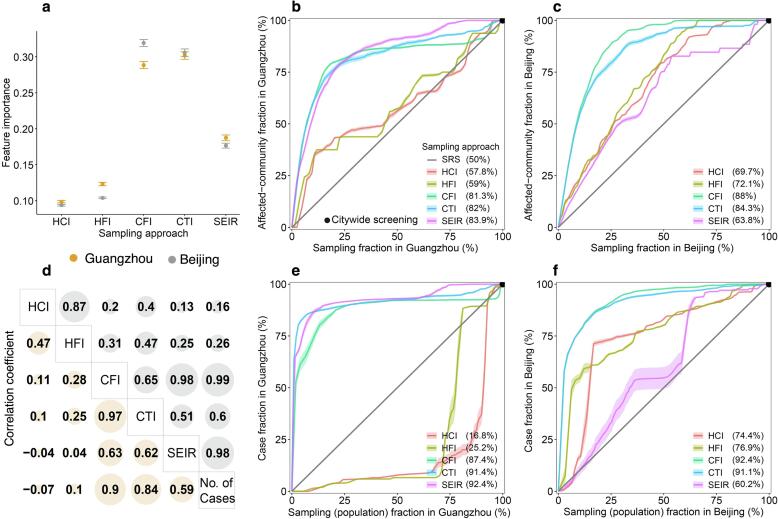
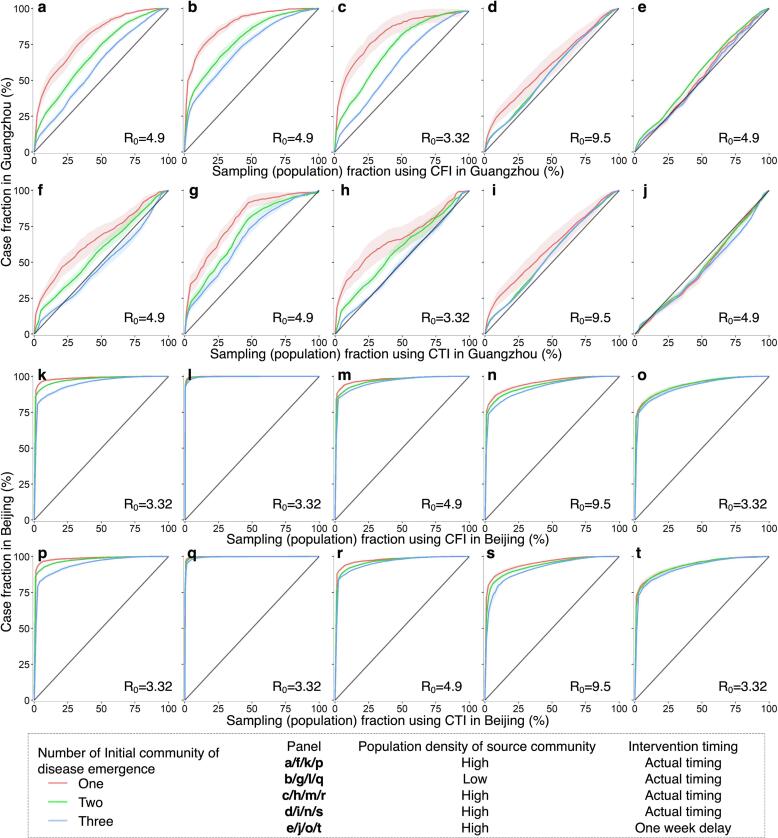
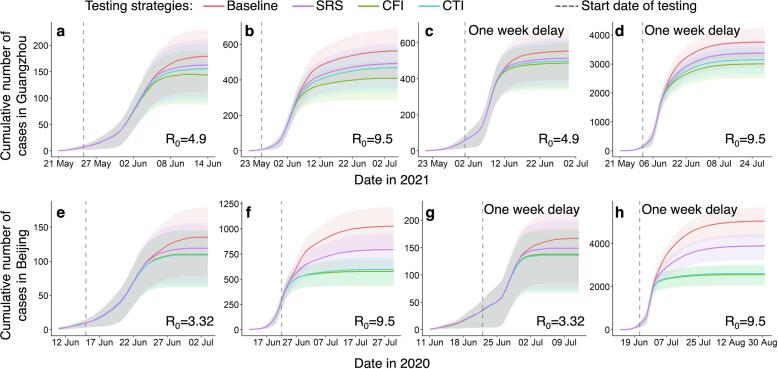
Timely and precise detection of emerging infections is imperative for effective outbreak management and disease control. Human mobility significantly influences the spatial transmission dynamics of infectious diseases. Spatial sampling, integrating the spatial structure of the target, holds promise as an approach for testing allocation in detecting infections, and leveraging information on individuals' movement and contact behavior can enhance targeting precision. This study introduces a spatial sampling framework informed by spatiotemporal analysis of human mobility data, aiming to optimize the allocation of testing resources for detecting emerging infections. Mobility patterns, derived from clustering point-of-interest and travel data, are integrated into four spatial sampling approaches at the community level. We evaluate the proposed mobility-based spatial sampling by analyzing both actual and simulated outbreaks, considering scenarios of transmissibility, intervention timing, and population density in cities. Results indicate that leveraging inter-community movement data and initial case locations, the proposed Case Flow Intensity (CFI) and Case Transmission Intensity (CTI)-informed spatial sampling enhances community-level testing efficiency by reducing the number of individuals screened while maintaining a high accuracy rate in infection identification. Furthermore, the prompt application of CFI and CTI within cities is crucial for effective detection, especially in highly contagious infections within densely populated areas. With the widespread use of human mobility data for infectious disease responses, the proposed theoretical framework extends spatiotemporal data analysis of mobility patterns into spatial sampling, providing a cost-effective solution to optimize testing resource deployment for containing emerging infectious diseases.
Keywords: Data analysis; Emerging infectious disease; Human mobility; Spatial sampling; Testing allocation.
© 2024 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Update of
-
Optimizing the detection of emerging infections using mobility-based spatial sampling.Res Sq [Preprint]. 2023 Nov 17:rs.3.rs-3597070. doi: 10.21203/rs.3.rs-3597070/v1. Res Sq. 2023. Update in: Int J Appl Earth Obs Geoinf. 2024 Jul;131:103949. doi: 10.1016/j.jag.2024.103949. PMID: 38014322 Free PMC article. Updated. Preprint.
References
-
- Aleta A., Martín-Corral D., Pastore y Piontti A., Ajelli M., Litvinova M., Chinazzi M., Dean N.E., Halloran M.E., Longini I.M., Jr, Merler S., Pentland A., Vespignani A., Moro E., Moreno Y. Modelling the impact of testing, contact tracing and household quarantine on second waves of COVID-19. Nat Hum Behav. 2020;4:964–971. doi: 10.1038/s41562-020-0931-9. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous