

Recent Advances in Minimally Invasive Management of Osteolytic Periacetabular Skeletal Metastases
- PMID: 38993598
- PMCID: PMC11236455
- DOI: 10.1055/s-0044-1787165
Recent Advances in Minimally Invasive Management of Osteolytic Periacetabular Skeletal Metastases
Abstract
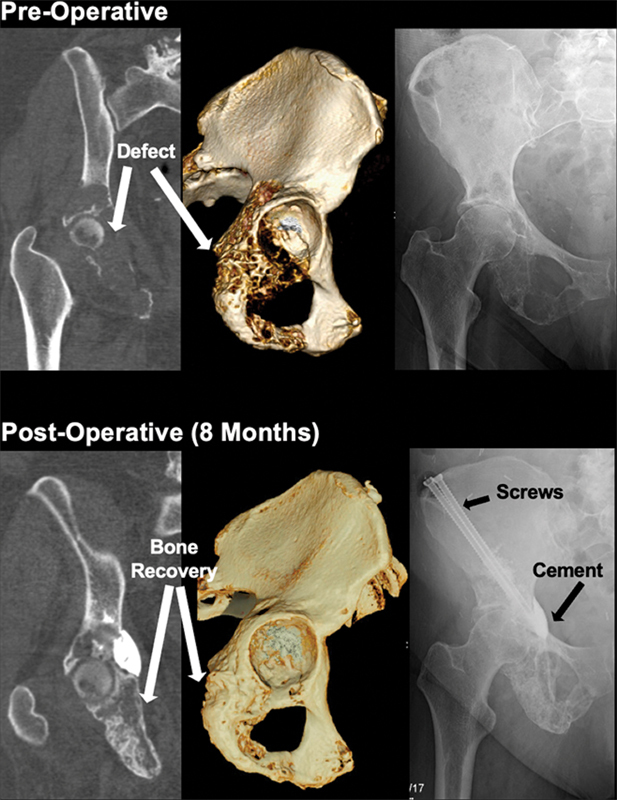
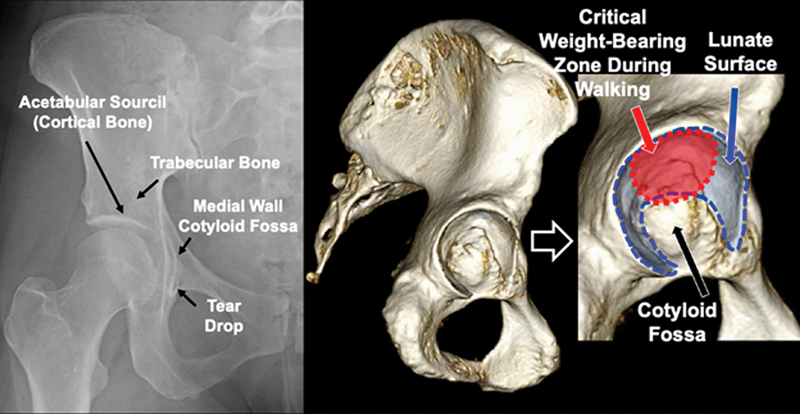
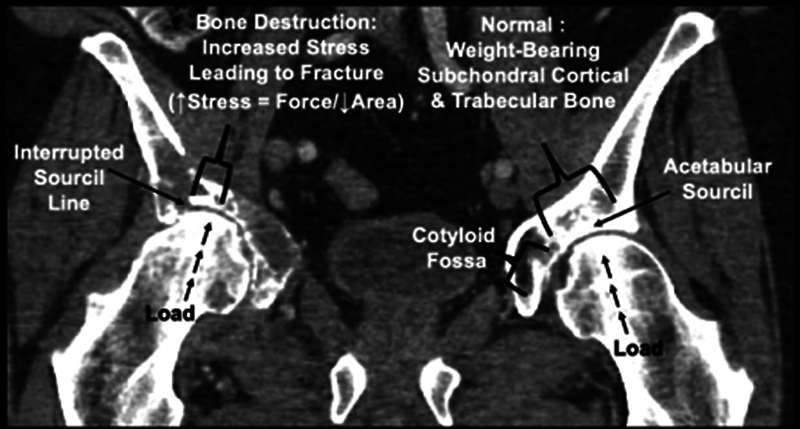
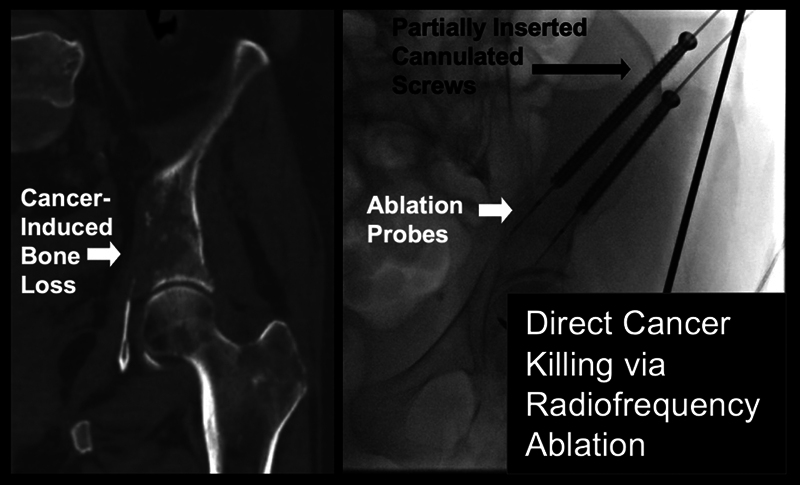
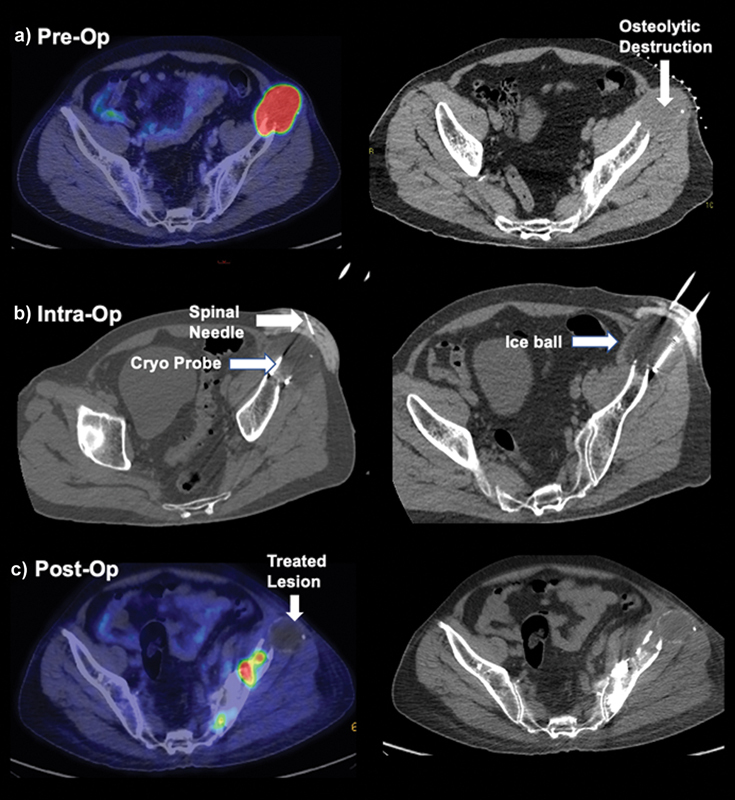
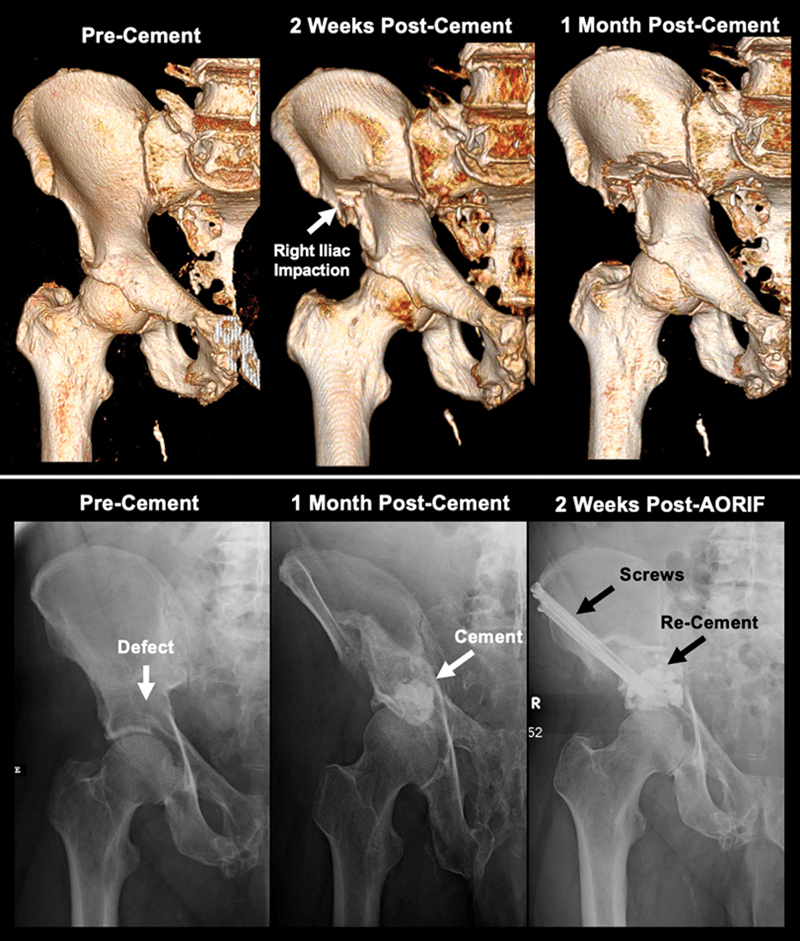
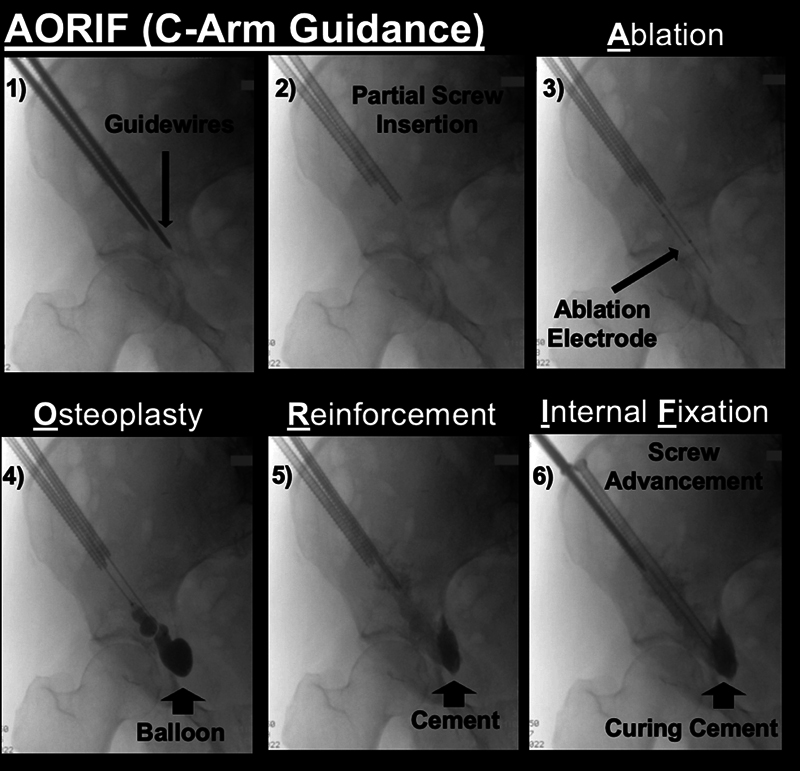
Painful skeletal osteolytic metastases, impending pathological fractures, and nondisplaced fractures present as a devastating clinical problem in advanced stage cancer patients. Open surgical approaches provide excellent mechanical stabilization but are often associated with high complication rates and slow recovery times. Percutaneous minimally invasive interventions have arisen as a pragmatic and logical treatment option for patients with late-stage cancer in whom open surgery may be contraindicated. These percutaneous interventions minimize soft tissue dissection, allow for the immediate initiation or resumption of chemotherapies, and present with fewer complications. This review provides the most up-to-date technical and conceptual framework for the minimally invasive management of osseous metastases with particular focus on periacetabular lesions. Fundamental topics discussed are as follows: (1) pathogenesis of cancer-induced bone loss and the importance of local cytoreduction to restore bone quality, (2) anatomy and biomechanics of the acetabulum as a weight-bearing zone, (3) overview of ablation options and cement/screw techniques, and (4) combinatorial approaches. Future studies should include additional studies with more long-term follow-up to better assess mechanical durability of minimally invasive interventions. An acetabulum-specific functional and pain scoring framework should be adopted to allow for better cross-study comparison.
Keywords: ablation; cement; metastases; percutaneous; periacetabular.
Thieme. All rights reserved.
Figures
References
-
- Walker R H. Pelvic reconstruction/total hip arthroplasty for metastatic acetabular insufficiency. Clin Orthop Relat Res. 1993;(294):170–175. - PubMed
-
- Enneking W F, Dunham W K. Resection and reconstruction for primary neoplasms involving the innominate bone. J Bone Joint Surg Am. 1978;60(06):731–746. - PubMed
-
- Harrington K D. The management of acetabular insufficiency secondary to metastatic malignant disease. J Bone Joint Surg Am. 1981;63(04):653–664. - PubMed
-
- Tillman R M, Myers G J, Abudu A T, Carter S R, Grimer R J. The three-pin modified ‘Harrington’ procedure for advanced metastatic destruction of the acetabulum. J Bone Joint Surg Br. 2008;90(01):84–87. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
