

A combination of risk stratification systems for thyroid nodules and cervical lymph nodes may improve the diagnosis and management of thyroid nodules
- PMID: 38993646
- PMCID: PMC11237952
- DOI: 10.3389/fonc.2024.1393414
A combination of risk stratification systems for thyroid nodules and cervical lymph nodes may improve the diagnosis and management of thyroid nodules
Abstract
Introduction: To assess the performance of the European Thyroid Association Thyroid Imaging and Reporting Data System (EU-TIRADS) and the Korean Thyroid Imaging Reporting and Data System (K-TIRADS), which combine risk stratification systems for thyroid nodules (TN-RSS) and cervical lymph nodes (LN-RSS) in diagnosing malignant and metastatic thyroid cancer in a single referral center.
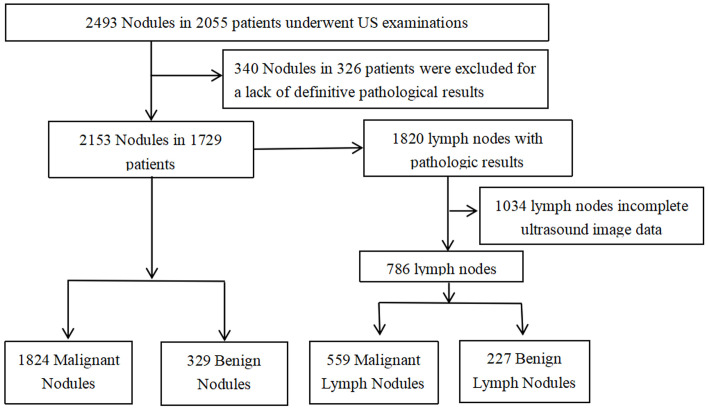
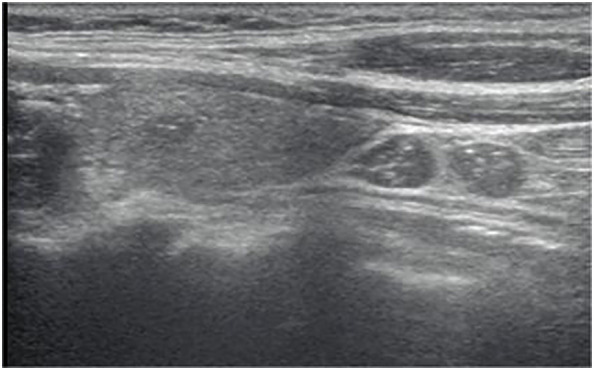
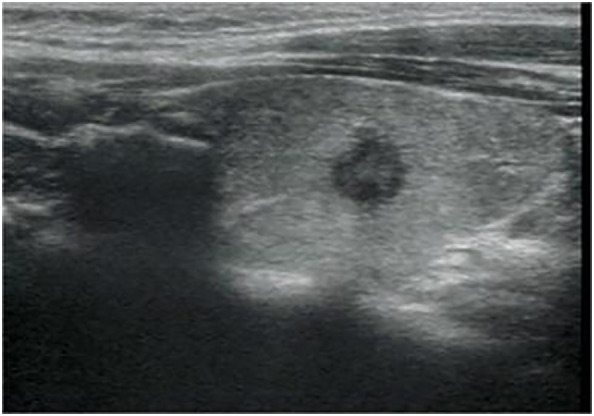
Methods: We retrospectively analyzed 2,055 consecutive patients who underwent thyroidectomy or fine-needle aspiration (FNA) from January 2021 to December 2022. TNs and LNs were categorized according to the ultrasonography (US) features of EU-TIRADS and K-TIRADS, respectively. The diagnostic performance and postponed malignancy rate (PMR) were compared with those of EU-TIRADS and K-TIRADS. PMR was defined as the number of patients with malignant nodules not recommended for biopsy among patients with cervical LN metastasis.
Results: According to the EU-TIRADS and K-TIRADS, for TN-RSS alone, there were no significant differences in sensitivity, specificity, accuracy, unnecessary FNA rate (UFR), missed malignancy rate (MMR), and PMR between the two TIRADSs (29.0% vs. 28.8%, 50.5% vs. 51.1%, 32.3% vs. 32.2%, 23.6% vs. 23.5%, 88.6% vs. 88.5%, and 54.2% vs. 54.5%, P > 0.05 for all). Combining the LN-RSS increased the diagnostic accuracy (42.7% vs. 32.3% in EU-TIRADS; 38.8% vs. 32.2% in K-TIRADS) and decreased the PMR (54.2% vs. 33.9% in EU-TIRADS; 54.5% vs. 39.3% in K-TIRADS). EU-TIRADS had higher sensitivity and accuracy and lower PMR than K-TIRADS (41.3% vs. 36.7%, 42.7% vs. 38.8%,33.9% vs. 39.3%, P < 0.05 for all).
Conclusions: A combination of TN-RSS and LN-RSS for the management of thyroid nodules may be associated with a reduction in PMR, with enhanced sensitivity and accuracy for thyroid cancers in EU-TIRADS and K-TIRADS. These results may offer a new direction for the detection of aggressive thyroid cancers.
Keywords: lymph nodes; management; risk stratification system; thyroid nodules; ultrasound.
Copyright © 2024 Xu, Yu, Cui, Huang, Fu and Cui.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources