

Gradual rewarming with a hemoglobin-based oxygen carrier improves viability of donation after circulatory death in rat livers
- PMID: 38993754
- PMCID: PMC11235298
- DOI: 10.3389/frtra.2024.1353124
Gradual rewarming with a hemoglobin-based oxygen carrier improves viability of donation after circulatory death in rat livers
Abstract
Background: Donation after circulatory death (DCD) grafts are vital for increasing available donor organs. Gradual rewarming during machine perfusion has proven effective in mitigating reperfusion injury and enhancing graft quality. Limited data exist on artificial oxygen carriers as an effective solution to meet the increasing metabolic demand with temperature changes. The aim of the present study was to assess the efficacy and safety of utilizing a hemoglobin-based oxygen carrier (HBOC) during the gradual rewarming of DCD rat livers.
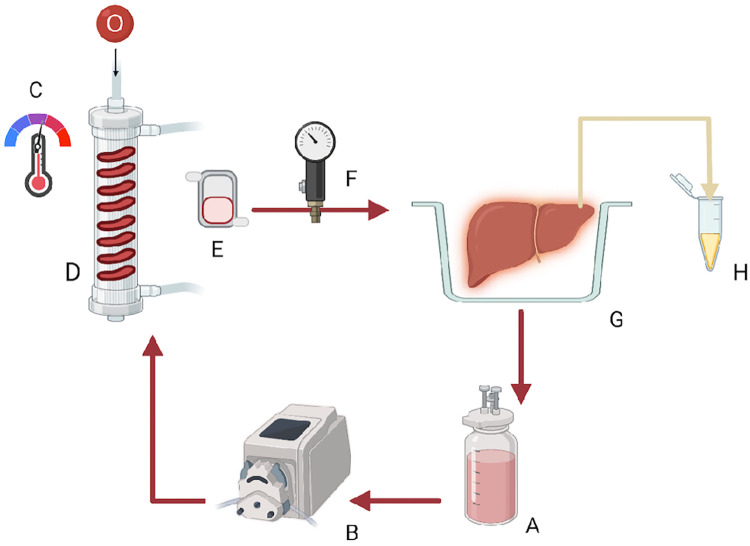
Methods: Liver grafts were procured after 30 min of warm ischemia. The effect of 90 min of oxygenated rewarming perfusion from ice cold temperatures (4 °C) to 37 °C with HBOC after cold storage was evaluated and the results were compared with cold storage alone. Reperfusion at 37 °C was performed to assess the post-preservation recovery.
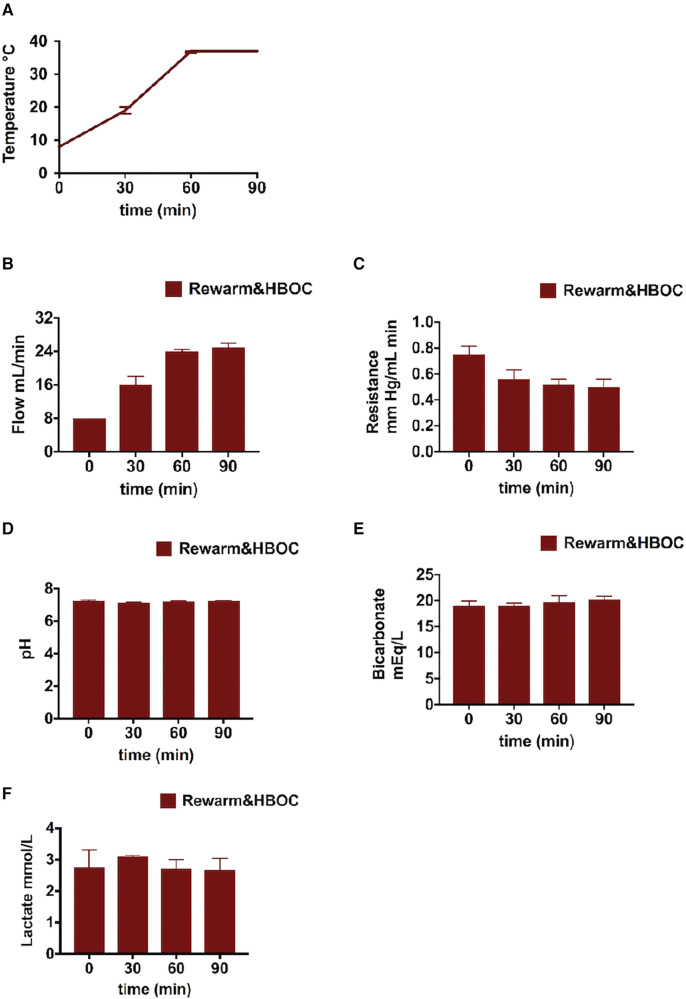
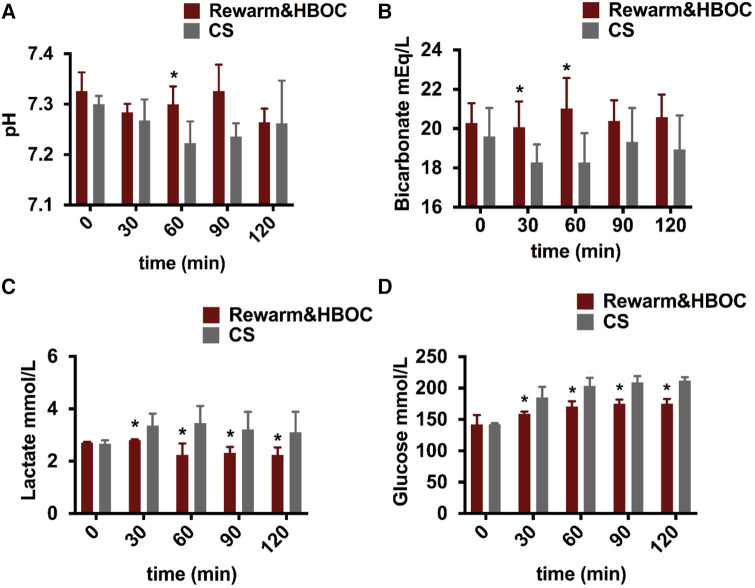
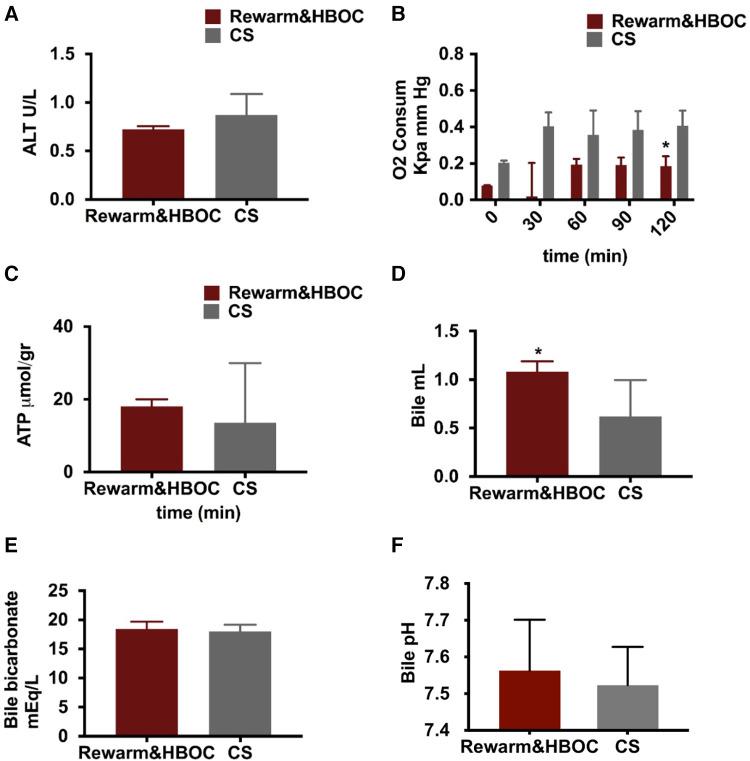
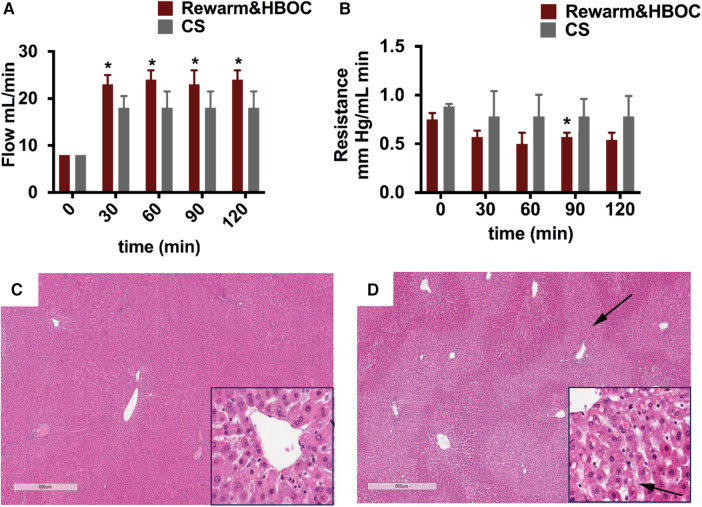
Results: Gradual rewarming with HBOC significantly enhanced recovery, demonstrated by markedly lower lactate levels and reduced vascular resistance compared to cold-stored liver grafts. Increased bile production in the HBOC group was noted, indicating improved liver function and bile synthesis capacity. Histological examination showed reduced cellular damage and better tissue preservation in the HBOC-treated livers compared to those subjected to cold storage alone.
Conclusion: This study suggests the safety of using HBOC during rewarming perfusion of rat livers as no harmful effect was detected. Furthermore, the viability assessment indicated improvement in graft function.
Keywords: HBOC; cold storage; donation after cardiac death (DCD); gradual rewarming; machine perfusion.
© 2024 Mahboub, Aburawi, Ozgur, Pendexter, Cronin, Lin, Jain, Karabacak, Karimian, Tessier, Markmann, Yeh and Uygun.
Conflict of interest statement
KU is inventor on pending patents relevant to this study, has a financial interest in Sylvatica Biotech, a company focused on developing organ preservation technology, whose interests are managed by the MGH and Mass General Brigham in accordance with their conflict of interest policies. ST and KU have several patent applications disclosures on extended organ preservation that may be relevant to this study. The HOBC-201 used in this study was provided by HBO2 Therapeutics LLC. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The authors declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures
References
-
- Quintini C, Muiesan P, Detry O, Gastaca M, de Jonge J, Clavien PA, et al. Early allograft dysfunction and complications in DCD liver transplantation: expert consensus statements from the international liver transplantation society. Transplantation. (2021) 105(8):1643–52. 10.1097/TP.0000000000003877 - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources