

The beneficial effects of conservative treatment with biofeedback and electrostimulation on pelvic floor disorders
- PMID: 38993823
- PMCID: PMC11236079
- DOI: 10.4103/tcmj.tcmj_174_23
The beneficial effects of conservative treatment with biofeedback and electrostimulation on pelvic floor disorders
Abstract
Objectives: Pelvic floor disorders (PFDs) such as stress urinary incontinence (SUI) and pelvic organ prolapse (POP) can be managed through conservative treatments, such as conservative management involving biofeedback (BF) and electrostimulation. This study aimed to investigate the therapeutic effects of conservative treatments on PFDs.
Materials and methods: A retrospective cohort study was conducted. Women with PFD who underwent 1-3 months of BF and electrostimulation between January 1, 2020, and January 31, 2021, were included in the study. BF treatment was administered using three sensors to monitor pelvic floor muscle activity, providing patients with immediate feedback and guidance on muscle exercises. One session lasted for 5-10 min. Electrostimulation treatment utilized a specially made pelvic belt with electrode sheets to stimulate and contract pelvic floor muscles passively. One session lasted for 15 min. Six therapies in 1 month were prescribed. Pre- and post-treatment Pelvic Floor Distress Inventory (PFDI-20) scores, including POP distress inventory 6 (POPDI-6), colorectal-anal distress inventory (CRAD-8), and urinary distress inventory 6 (UDI-6) scores, were compared. Subgroup analysis by age, menopause, body mass index (BMI), and child delivery mode was performed.
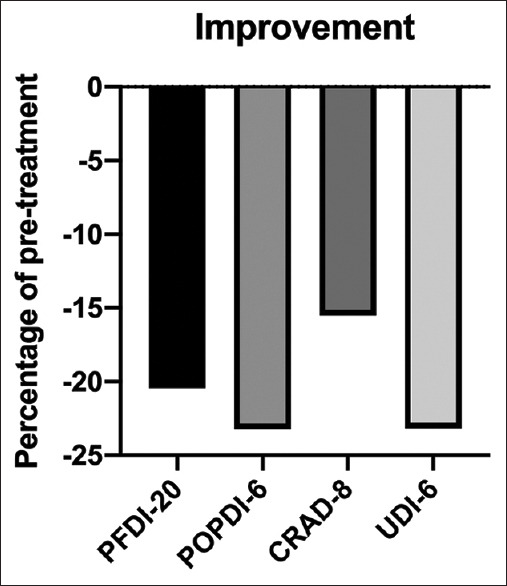
Results: The study included 51 women with PFDs (SUI, POP, frequency or urgency or nocturia, and pain) treated with BF and electrostimulation, with a mean age of 49.94 ± 13.63 years. Sixteen patients (37.1%) were menopausal, with a mean menopause age of 50 ± 5.20 years. Twenty-six patients (68.4%) had a history of normal vaginal delivery. The mean PFDI-20 scores before and after treatment were 32.67 (standard deviation [SD] 10.05) and 25.99 (SD 9.61), respectively (P < 0.001). This decrease in scores reflected an improvement in subjective perceptions of symptoms and quality of life. The POPDI-6, CRAD-8, and UDI-6 scores significantly decreased after treatment. Subgroup analysis of scores change regarding age, menopause, BMI, and child delivery mode was not statistically significant.
Conclusion: The study demonstrated the effectiveness of BF and electrostimulation for treating women with PFDs. The findings contributed to the understanding of treatment duration, patient characteristics, and the potential benefits of a multimodal approach. Moreover, the study's diverse participant population and the use of validated outcome measures enhance the generalizability and scientific rigor of the findings.
Keywords: Biofeedback; Electrostimulation; Pelvic organ prolapse; Pelvic pain; Stress urinary incontinence.
Copyright: © 2023 Tzu Chi Medical Journal.
Conflict of interest statement
Dr.Dah-Ching Ding, an editorial board member at Tzu Chi Medical Journal, had no role in the peer review process of or decision to publish this article. The other authors declared no conflicts of interest in writing this paper.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous