

The Management of Cardiogenic Shock From Diagnosis to Devices: A Narrative Review
- PMID: 38993934
- PMCID: PMC11238736
- DOI: 10.1016/j.chstcc.2024.100071
The Management of Cardiogenic Shock From Diagnosis to Devices: A Narrative Review
Abstract
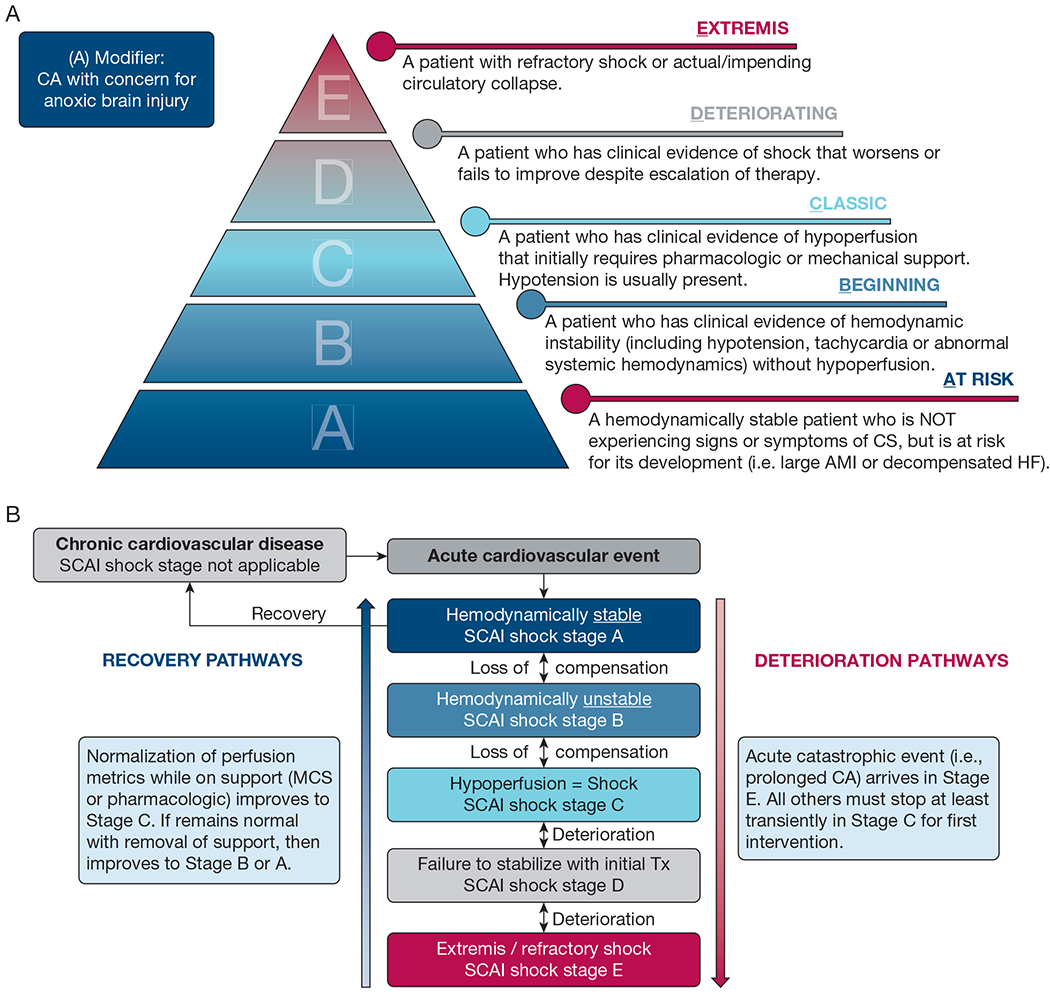
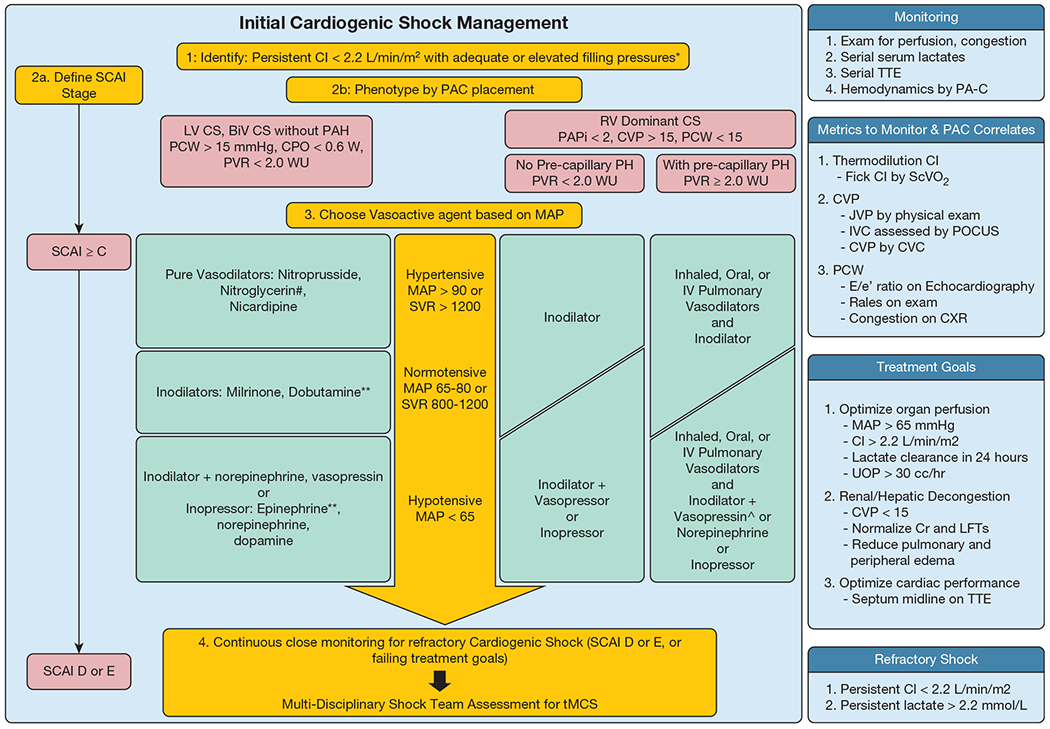
Cardiogenic shock (CS) is a heterogenous syndrome broadly characterized by inadequate cardiac output leading to tissue hypoperfusion and multisystem organ dysfunction that carries an ongoing high mortality burden. The management of CS has advanced rapidly, especially with the incorporation of temporary mechanical circulatory support (tMCS) devices. A thorough understanding of how to approach a patient with CS and to select appropriate monitoring and treatment paradigms is essential in modern ICUs. Timely characterization of CS severity and hemodynamics is necessary to optimize outcomes, and this may be performed best by multidisciplinary shock-focused teams. In this article, we provide a review of CS aimed to inform both the cardiology-trained and non-cardiology-trained intensivist provider. We briefly describe the causes, pathophysiologic features, diagnosis, and severity staging of CS, focusing on gathering key information that is necessary for making management decisions. We go on to provide a more detailed review of CS management principles and practical applications, with a focus on tMCS. Medical management focuses on appropriate medication therapy to optimize perfusion-by enhancing contractility and minimizing afterload-and to facilitate decongestion. For more severe CS, or for patients with decompensating hemodynamic status despite medical therapy, initiation of the appropriate tMCS increasingly is common. We discuss the most common devices currently used for patients with CS-phenotyping patients as having left ventricular failure, right ventricular failure, or biventricular failure-and highlight key available data and particular points of consideration that inform tMCS device selection. Finally, we highlight core components of sedation and respiratory failure management for patients with CS.
Keywords: cardiogenic shock; cardiogenic shock severity classification; mechanical circulatory support.
Conflict of interest statement
Financial/Nonfinancial Disclosures None declared.
Figures
Similar articles
-
Tailored Approach to Temporary Mechanical Circulatory Support for Cardiogenic Shock: Strategies to Facilitate Patient Mobilization.Curr Cardiol Rep. 2025 Jan 10;27(1):14. doi: 10.1007/s11886-024-02152-0. Curr Cardiol Rep. 2025. PMID: 39792281 Review.
-
Review of Pathophysiology of Cardiogenic Shock and Escalation of Mechanical Circulatory Support Devices.Curr Cardiol Rep. 2023 Apr;25(4):213-227. doi: 10.1007/s11886-023-01843-4. Epub 2023 Feb 27. Curr Cardiol Rep. 2023. PMID: 36847990 Review.
-
Evolving Concepts in Diagnosis and Management of Cardiogenic Shock.Am J Cardiol. 2018 Sep 15;122(6):1104-1110. doi: 10.1016/j.amjcard.2018.05.040. Epub 2018 Jun 22. Am J Cardiol. 2018. PMID: 30072134 Review.
-
The Role of a Cardiogenic Shock Team in Decision Making Surrounding Mechanical Circulatory Support.Can J Cardiol. 2025 Apr;41(4):682-690. doi: 10.1016/j.cjca.2025.02.002. Epub 2025 Feb 7. Can J Cardiol. 2025. PMID: 39922308 Review.
-
From medical therapy to mechanical support: strategies for device selection and implantation techniques.Eur Heart J Suppl. 2023 Dec 13;25(Suppl I):I11-I18. doi: 10.1093/eurheartjsupp/suad128. eCollection 2023 Dec. Eur Heart J Suppl. 2023. PMID: 38093767 Free PMC article.
Cited by
-
Sepsis-induced cardiogenic shock: controversies and evidence gaps in diagnosis and management.J Intensive Care. 2025 Jan 2;13(1):1. doi: 10.1186/s40560-024-00770-y. J Intensive Care. 2025. PMID: 39748440 Free PMC article. Review.
-
Case report: ST-elevation myocardial infarction complications. How far will you go?Future Cardiol. 2025 Mar;21(4):217-221. doi: 10.1080/14796678.2025.2471732. Epub 2025 Feb 26. Future Cardiol. 2025. PMID: 40011200
-
Modelling and Simulation of the Interactions Between the Cardiovascular System and the Combined Use of VA ECMO and IABP: Comparison Between Peripheral and Central Configurations.Bioengineering (Basel). 2025 May 17;12(5):540. doi: 10.3390/bioengineering12050540. Bioengineering (Basel). 2025. PMID: 40428159 Free PMC article.
-
Myocardial Recovery in Cardiogenic Shock.Methodist Debakey Cardiovasc J. 2024 Aug 20;20(4):64-75. doi: 10.14797/mdcvj.1383. eCollection 2024. Methodist Debakey Cardiovasc J. 2024. PMID: 39184158 Free PMC article. Review.
References
-
- van Diepen S, Katz JN, Albert NM, et al. Contemporary management of cardiogenic shock: a scientific statement from the American Heart Association. Circulation. 2017;136(16):e232–e268. - PubMed
-
- Kapur NK, Kanwar M, Sinha SS, et al. Criteria for defining stages of cardiogenic shock severity. J Am Coll Cardiol. 2022;80(3):185–198. - PubMed
-
- Jentzer JC, Ahmed AM, Vallabhajosyula S, et al. Shock in the cardiac intensive care unit: changes in epidemiology and prognosis over time. Am Heart J. 2021;232:94–104. - PubMed
-
- Thiele H, Akin I, Sandri M, et al. PCI Strategies in patients with acute myocardial infarction and cardiogenic shock. N Engl J Med. 2017;377(25):2419–2432. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources