

A Systematic Review of Outcome Reporting, Definition and Measurement Heterogeneity in Non-Muscle Invasive Bladder Cancer Effectiveness Trials of Adjuvant, Prophylactic Treatment After Transurethral Resection
- PMID: 38994538
- PMCID: PMC11181687
- DOI: 10.3233/BLC-201510
A Systematic Review of Outcome Reporting, Definition and Measurement Heterogeneity in Non-Muscle Invasive Bladder Cancer Effectiveness Trials of Adjuvant, Prophylactic Treatment After Transurethral Resection
Abstract
Background: Heterogenous outcome reporting in non-muscle-invasive bladder cancer (NMIBC) effectiveness trials of adjuvant treatment after transurethral resection (TURBT) has been noted in systematic reviews (SRs). This hinders comparing results across trials, combining them in meta-analyses, and evidence-based decision-making for patients and clinicians.
Objective: We aimed to systematically review the extent of reporting and definition heterogeneity.
Methods: We included randomized controlled trials (RCTs) identified from SRs comparing adjuvant treatments after TURBT or TURBT alone in patients with NMIBC (with or without carcinoma in situ) published between 2000-2020. Abstracts and full texts were screened independently by two reviewers. Data were extracted by one reviewer and checked by another.
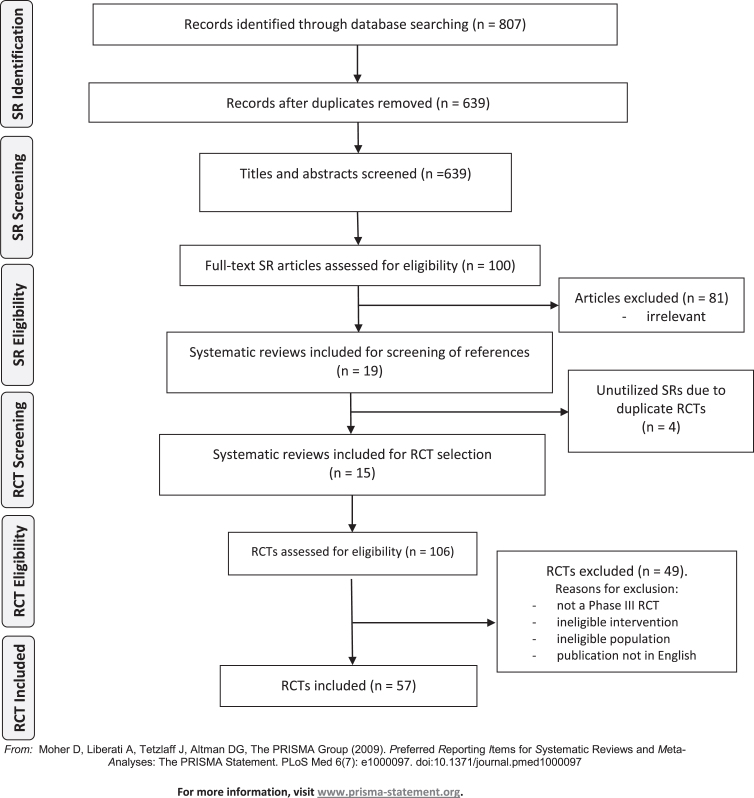
Results: We screened 807 abstracts; from 15 SRs, 57 RCTs were included. Verbatim outcome names were coded to standard outcome names and organised using the Williamson and Clarke taxonomy. Recurrence (98%), progression (74%), treatment response (in CIS studies) (40%), and adverse events (77%) were frequently reported across studies. However, overall (33%) and cancer-specific (33%) survival, treatment completion (17%) and treatment change (37%) were less often reported. Quality of Life (3%) and economic outcomes (2%) were rarely reported. Heterogeneity was evident throughout, particularly in the definitions of progression and recurrence, and how CIS patients were handled in the analysis of studies with predominantly papillary patients, highlighting further issues with the definition of recurrence and progression vs treatment response for CIS patients. Data reporting was also inconsistent, with some trials reporting event rates at various time-points and others reporting time-to-event with or without Hazard Ratios. Adverse events were inconsistently reported. QoL data was absent in most trials.
Conclusions: Heterogenous outcome reporting is evident in NMIBC effectiveness trials. This has profound implications for meta-analyses, SRs and evidence-based treatment decisions. A core outcome set is required to reduce heterogeneity.
Patient summary: This systematic review found inconsistencies in outcome definitions and reporting, pointing out the urgent need for a core outcome set to help improve evidence-based treatment decisions.
Keywords: Outcome reporting heterogeneity; TURBT; core outcome sets; non-muscle-invasive bladder cancer (NMIBC); systematic review.
© 2021 – IOS Press. All rights reserved.
Conflict of interest statement
Erik Veskimae – Has no conflict of interest to report. Selvarani Subbarayan – Has no conflict of interest to report. Riccardo Campi – Has no conflict of interest to report. Domitille Carron – Has no conflict of interest to report. Muhammad Imran Omar – Has no conflict of interest to report. Cathy Yuan – Has no conflict of interest to report. Konstantinos Dimitropoulos – Has no conflict of interest to report. Mieke Van Hemelrijck – Has no conflict of interest to report. Richard T. Bryan – Reports other from Janssen EMEA, grants from UroGen Pharma, grants from QED Therapeutics, outside the submitted work. James N’Dow – Has no conflict of interest to report. Marek Babjuk – Has no conflict of interest to report. J. Alfred Witjes – Has no conflict of interest to report. Richard Sylvester – Has no conflict of interest to report. Steven MacLennan – Has no conflict of interest to report.
Figures
Similar articles
-
Enhanced Visualization Methods for First Transurethral Resection of Bladder Tumour in Suspected Non-muscle-invasive Bladder Cancer: A Health Technology Assessment.Ont Health Technol Assess Ser. 2021 Aug 12;21(12):1-123. eCollection 2021. Ont Health Technol Assess Ser. 2021. PMID: 34484486 Free PMC article.
-
The future of Cochrane Neonatal.Early Hum Dev. 2020 Nov;150:105191. doi: 10.1016/j.earlhumdev.2020.105191. Epub 2020 Sep 12. Early Hum Dev. 2020. PMID: 33036834
-
A Systematic Review of Heterogeneity in Outcome Definition and Reporting in Localised Renal Cancer.Eur Urol Open Sci. 2022 Dec 15;48:1-11. doi: 10.1016/j.euros.2022.11.014. eCollection 2023 Feb. Eur Urol Open Sci. 2022. PMID: 36578462 Free PMC article. Review.
-
Prospective Assessment of Vesical Imaging Reporting and Data System (VI-RADS) and Its Clinical Impact on the Management of High-risk Non-muscle-invasive Bladder Cancer Patients Candidate for Repeated Transurethral Resection.Eur Urol. 2020 Jan;77(1):101-109. doi: 10.1016/j.eururo.2019.09.029. Epub 2019 Nov 5. Eur Urol. 2020. PMID: 31699526
-
The Impact of Restaging Transurethral Resection of Bladder Tumor on Survival Parameters in T1 Nonmuscle-Invasive Bladder Cancer: Systematic Review and Meta-Analysis.J Endourol. 2020 Aug;34(8):795-804. doi: 10.1089/end.2020.0301. Epub 2020 Jun 3. J Endourol. 2020. PMID: 32336149
Cited by
-
Intermediate and high-risk non-muscle-invasive bladder cancer: an overview of epidemiology, burden, and unmet needs.Front Oncol. 2023 Jun 2;13:1170124. doi: 10.3389/fonc.2023.1170124. eCollection 2023. Front Oncol. 2023. PMID: 37333804 Free PMC article. Review.
-
Core outcome sets in cancer clinical trials: current status and future opportunities-an EORTC perspective.Trials. 2025 Apr 9;26(1):129. doi: 10.1186/s13063-025-08812-y. Trials. 2025. PMID: 40205620 Free PMC article.
-
Impact of Effective Intravesical Therapies on Quality of Life in Patients with Non-Muscle Invasive Bladder Cancer: A Systematic Review.Int J Environ Res Public Health. 2022 Aug 30;19(17):10825. doi: 10.3390/ijerph191710825. Int J Environ Res Public Health. 2022. PMID: 36078542 Free PMC article.
References
-
- Brierley J, Gospodarowicz M, Wittekind C. TNM Classification of Malignant Tumours, 8th Edition. Wiley-Blackwell; 2017.
Publication types
LinkOut - more resources
Full Text Sources
