

Global, regional, and national burden of gout, 1990-2020, and projections to 2050: a systematic analysis of the Global Burden of Disease Study 2021
- PMID: 38996590
- PMCID: PMC11263476
- DOI: 10.1016/S2665-9913(24)00117-6
Global, regional, and national burden of gout, 1990-2020, and projections to 2050: a systematic analysis of the Global Burden of Disease Study 2021
Erratum in
-
Correction to Lancet Rheumatol 2024; 6: e507-17.Lancet Rheumatol. 2024 Nov;6(11):e749. doi: 10.1016/S2665-9913(24)00303-5. Epub 2024 Sep 27. Lancet Rheumatol. 2024. PMID: 39348836 Free PMC article. No abstract available.
Abstract
Background: Gout is an inflammatory arthritis manifesting as acute episodes of severe joint pain and swelling, which can progress to chronic tophaceous or chronic erosive gout, or both. Here, we present the most up-to-date global, regional, and national estimates for prevalence and years lived with disability (YLDs) due to gout by sex, age, and location from the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2021, as well as forecasted prevalence to 2050.
Methods: Gout prevalence and YLDs from 1990 to 2020 were estimated by drawing on population-based data from 35 countries and claims data from the USA and Taiwan (province of China). Nested Bayesian meta-regression models were used to estimate prevalence and YLDs due to gout by age, sex, and location. Prevalence was forecast to 2050 with a mixed-effects model.
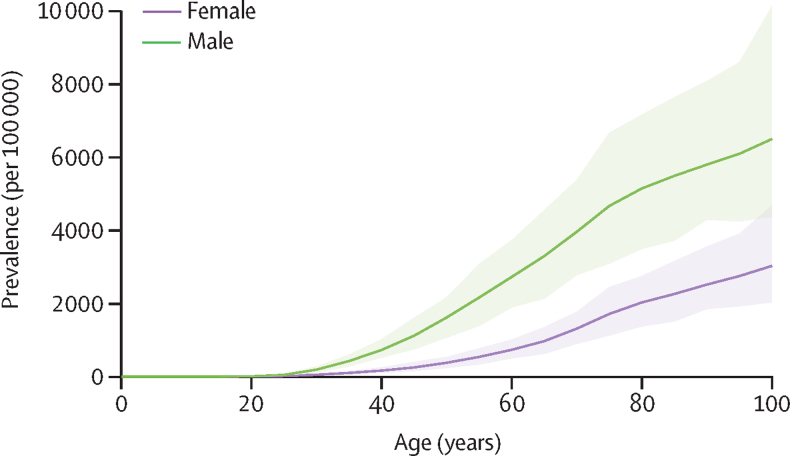
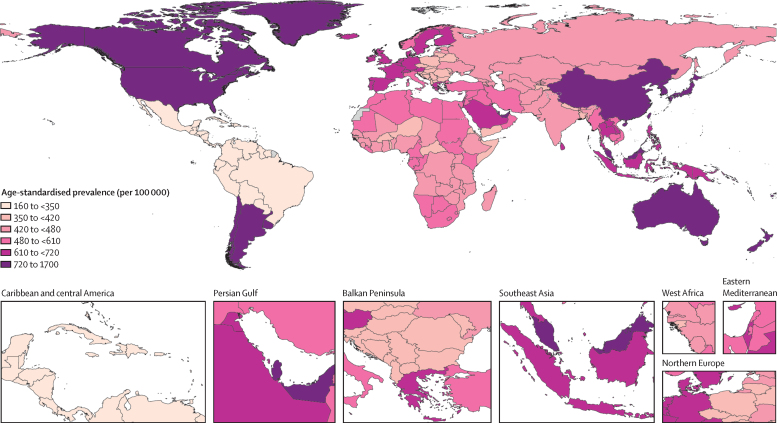
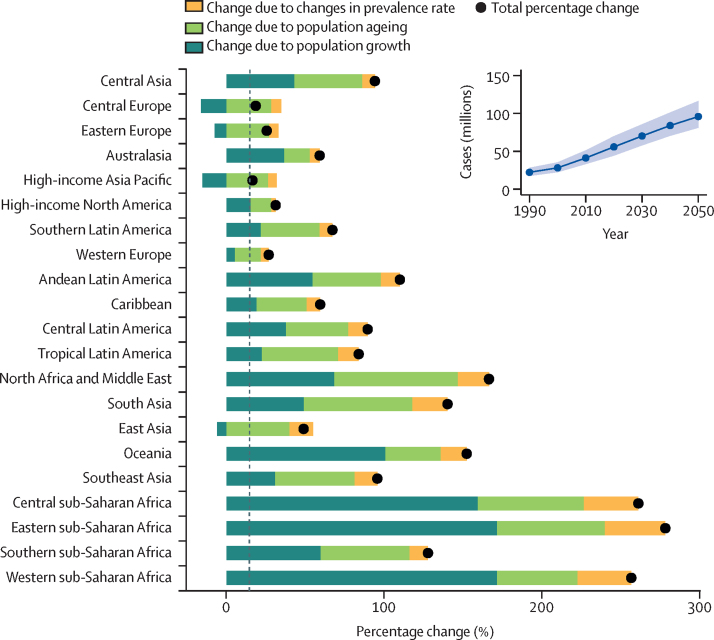
Findings: In 2020, 55·8 million (95% uncertainty interval 44·4-69·8) people globally had gout, with an age-standardised prevalence of 659·3 (525·4-822·3) per 100 000, an increase of 22·5% (20·9-24·2) since 1990. Globally, the prevalence of gout in 2020 was 3·26 (3·11-3·39) times higher in males than in females and increased with age. The total number of prevalent cases of gout is estimated to reach 95·8 million (81·1-116) in 2050, with population growth being the largest contributor to this increase and only a very small contribution from the forecasted change in gout prevalence. Age-standardised gout prevalence in 2050 is forecast to be 667 (531-830) per 100 000 population. The global age-standardised YLD rate of gout was 20·5 (14·4-28·2) per 100 000 population in 2020. High BMI accounted for 34·3% (27·7-40·6) of YLDs due to gout and kidney dysfunction accounted for 11·8% (9·3-14·2).
Interpretation: Our forecasting model estimates that the number of individuals with gout will increase by more than 70% from 2020 to 2050, primarily due to population growth and ageing. With the association between gout disability and high BMI, dietary and lifestyle modifications focusing on bodyweight reduction are needed at the population level to reduce the burden of gout along with access to interventions to prevent and control flares. Despite the rigour of the standardised GBD methodology and modelling, in many countries, particularly low-income and middle-income countries, estimates are based on modelled rather than primary data and are also lacking severity and disability estimates. We strongly encourage the collection of these data to be included in future GBD iterations.
Funding: Bill & Melinda Gates Foundation and the Global Alliance for Musculoskeletal Health.
Copyright © 2024 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests R Buchbinder reports grants or contracts from Australian National Health and Medical Research Council, Australian Government, Arthritis Australia, HCF Foundation, Cabrini Foundation; royalties from Wolters Klewer Health for authorship of the chapterPlantar fasciitis in UpToDate; all outside the submitted work. S Das reports voluntary member and leadership of the Association of Diagnostic and Laboratory Medicine and Women in Global Health, outside the submitted work. D R Kopansky-Giles reports support for the present manuscript from Global Alliance for Musculoskeletal Health; leadership or fiduciary roles in board, society, committee or advocacy groups, paid or unpaid, with Global Alliance for Musculoskeletal Health with the International Coordinating Council and World Spine Care, Canada, as a member of the Canadian Board of Directors; all outside the submitted work. K Krishan reports non-financial support from the UGC Centre of Advanced Study, CAS II (awarded to the Department of Anthropology, Panjab University, Chandigarh, India), outside the submitted work. L M March reports grants or contracts from National Health and Medical Research Council (NHMRC) Australian Government for Centre of Research Excellence for Better Outcomes in Inflammatory Arthritis, Medical Research Future Fund (MRFF) Australian Government for a Biologic Tapering trial in Adults with rheumatoid arthritis and psoriatic arthritis, and MRFF Australian Government for a biologic tapering trial in children with juvenile idiopathic arthritis; royalties from Wolters Klewer Health for authorship of the chapter Epidemiology and risk factors for osteoarthritis in UpToDate; royalties from Elsevier for being co-editor of The Musculoskeletal System, 3rd Edn, 2022; participation on a Data Safety Monitoring Board (DSMB) or Advisory Board with NHMRC Australian Government as a pro-bono member of DSMB for an investigator initiated text message study for low back pain; leadership or fiduciary roles in board, society, committee or advocacy groups, paid or unpaid, with Australian Rheumatology Association as a pro-bono Chair Research Advisory Committee and Global Alliance for MSK Health – Global Alliance for Musculoskeletal Health as a pro-bono Executive Committee member; all outside the submitted work. All other authors declare no competing interests.
Figures
References
-
- Singh JA, Gaffo A. Gout epidemiology and comorbidities. Semin Arthritis Rheum. 2020;50:S11–S16. - PubMed
-
- Dalbeth N, Gosling AL, Gaffo A, Abhishek A. Gout. Lancet. 2021;397:1843–1855. - PubMed
-
- Kuo C-F, Grainge MJ, Zhang W, Doherty M. Global epidemiology of gout: prevalence, incidence and risk factors. Nat Rev Rheumatol. 2015;11:649–662. - PubMed
-
- Zhu Y, Pandya BJ, Choi HK. Comorbidities of gout and hyperuricemia in the US general population: NHANES 2007–2008. Am J Med. 2012;125:679. 87.e1. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
