

Distinct neurodevelopmental and epileptic phenotypes associated with gain- and loss-of-function GABRB2 variants
- PMID: 38996765
- PMCID: PMC11296288
- DOI: 10.1016/j.ebiom.2024.105236
Distinct neurodevelopmental and epileptic phenotypes associated with gain- and loss-of-function GABRB2 variants
Abstract
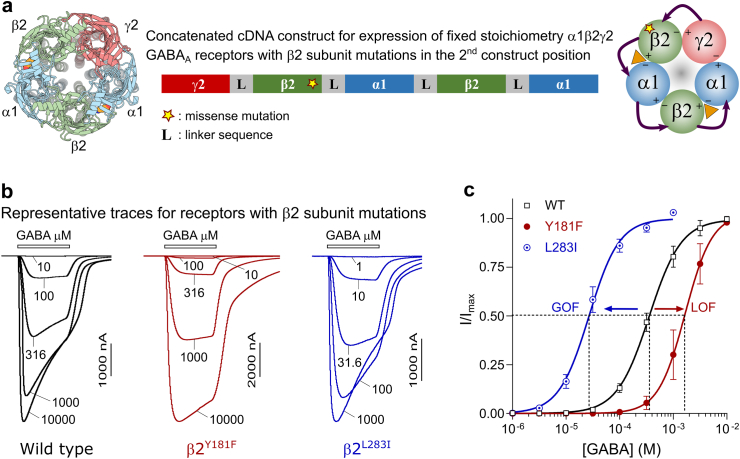
Background: Variants in GABRB2, encoding the β2 subunit of the γ-aminobutyric acid type A (GABAA) receptor, can result in a diverse range of conditions, ranging from febrile seizures to severe developmental and epileptic encephalopathies. However, the mechanisms underlying the risk of developing milder vs more severe forms of disorder remain unclear. In this study, we conducted a comprehensive genotype-phenotype correlation analysis in a cohort of individuals with GABRB2 variants.
Methods: Genetic and electroclinical data of 42 individuals harbouring 26 different GABRB2 variants were collected and accompanied by electrophysiological analysis of the effects of the variants on receptor function.
Findings: Electrophysiological assessments of α1β2γ2 receptors revealed that 25/26 variants caused dysfunction to core receptor properties such as GABA sensitivity. Of these, 17 resulted in gain-of-function (GOF) while eight yielded loss-of-function traits (LOF). Genotype-phenotype correlation analysis revealed that individuals harbouring GOF variants suffered from severe developmental delay/intellectual disability (DD/ID, 74%), movement disorders such as dystonia or dyskinesia (59%), microcephaly (50%) and high risk of early mortality (26%). Conversely, LOF variants were associated with milder disease manifestations. Individuals with these variants typically exhibited fever-triggered seizures (92%), milder degrees of DD/ID (85%), and maintained ambulatory function (85%). Notably, severe movement disorders or microcephaly were not reported in individuals with loss-of-function variants.
Interpretation: The data reveals that genetic variants in GABRB2 can lead to both gain and loss-of-function, and this divergence is correlated with distinct disease manifestations. Utilising this information, we constructed a diagnostic flowchart that aids in predicting the pathogenicity of recently identified variants by considering clinical phenotypes.
Funding: This work was funded by the Australian National Health & Medical Research Council, the Novo Nordisk Foundation and The Lundbeck Foundation.
Keywords: Dystonia; Epilepsy; GABA(A) receptors; Gain-of-function; Movement disorders; Seizures.
Copyright © 2024 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests SOR is the chair of the Young Epilepsy Section, ILAE, and has received consulting fees from Biopas-UCB, support for attending meetings and/or travel from Mythotherapies, and speaker fees from Abbott, LivaNova, Sanofi, Biopas-UCB and Nutricia. MT has received consulting fees from Biomarin, support for attending meetings and/or travel from Biomarin and Jazz Pharmaceuticals, and participated in Data Safety Monitoring Boards or Advisory Boards for Biocodex. SA is the deputy editor of Epilepsia, and has received consulting fees from UCB, Xenon, Encoded Therapeutics, EISAI, Stoke, Proveca, speaker fees from Biocodex, EISAI, Jazz Pharmaceuticals, Neuraxpharm, Nutricia and UCB and participated in Data Safety Monitoring Boards or Advisory Boards for GRIN Therapeutics. JK has received consulting fees from Biomarin, support for attending meetings and/or travel from Biomarin and Jazz Pharmaceuticals, and participated in Data Safety Monitoring Boards or Advisory Boards for Biocodex. SW has received consulting fees from UCB, Knopp Biosciences, Encoded Therapeutics, Roche, support for attending meetings and/or travel from Angelini Pharma, and participated in Data Safety Monitoring Boards or Advisory Boards for Angelini Pharma and Xenon Pharmaceuticals. NS has received consulting fees from Biomarin, support for attending meetings and/or travel from Biomarin and Jazz Pharmaceuticals, and participated in Data Safety Monitoring Boards or Advisory Boards for Biocodex. PB has received consulting fees from LivaNova, EISAI, Jazz Pharmaceuticals, Angelini Pharma and support for attending meetings and/or travel from Angelini Pharma and EISAI. RSM has received consulting fees from UCB, Orion, Saniona, Immedica and Atalanta, and speaker fees from EISAI, Angelini Pharma, Jazz Pharmaceuticals, Orion and UCB. PC is Executive Vice President, Research at the company Saniona in Denmark. The remaining authors declare no competing interests.
Figures






References
-
- Baulac S., Huberfeld G., Gourfinkel-An I., et al. First genetic evidence of GABA(A) receptor dysfunction in epilepsy: a mutation in the gamma2-subunit gene. Nat Genet. 2001;28(1):46–48. - PubMed
-
- Hirose S. Mutant GABA(A) receptor subunits in genetic (idiopathic) epilepsy. Prog Brain Res. 2014;213:55–85. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
