

Disruption of neural periodicity predicts clinical response after deep brain stimulation for obsessive-compulsive disorder
- PMID: 38997607
- PMCID: PMC11485242
- DOI: 10.1038/s41591-024-03125-0
Disruption of neural periodicity predicts clinical response after deep brain stimulation for obsessive-compulsive disorder
Erratum in
-
Author Correction: Disruption of neural periodicity predicts clinical response after deep brain stimulation for obsessive-compulsive disorder.Nat Med. 2025 May;31(5):1716. doi: 10.1038/s41591-025-03667-x. Nat Med. 2025. PMID: 40140624 Free PMC article. No abstract available.
Abstract
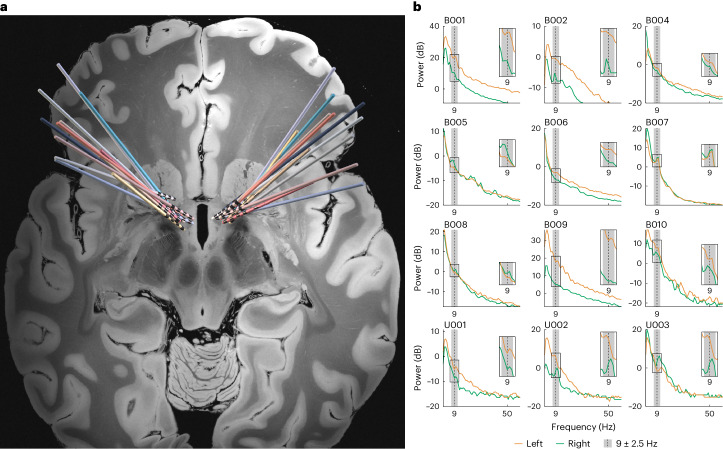
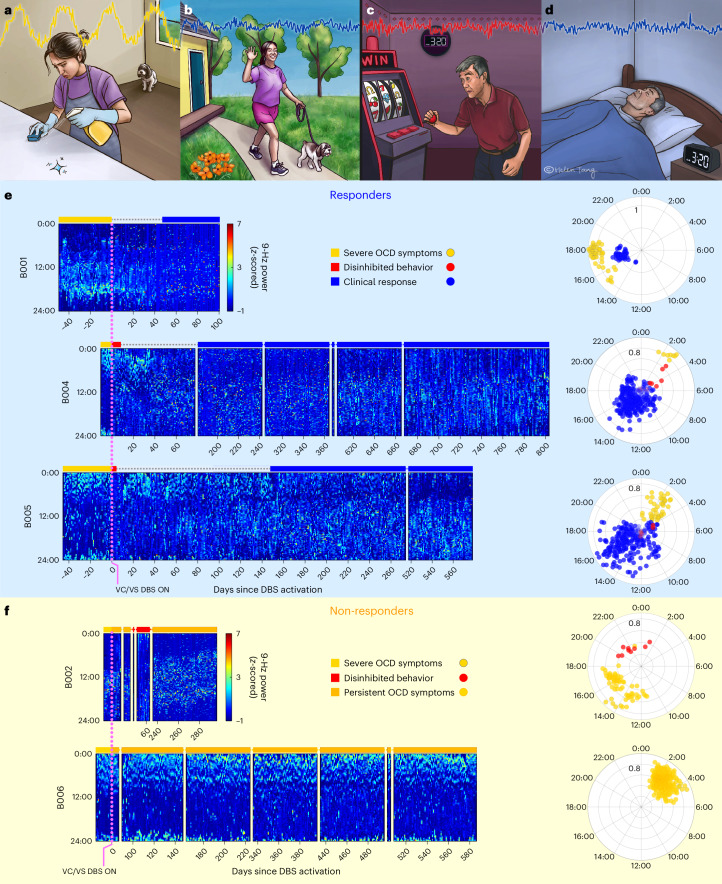
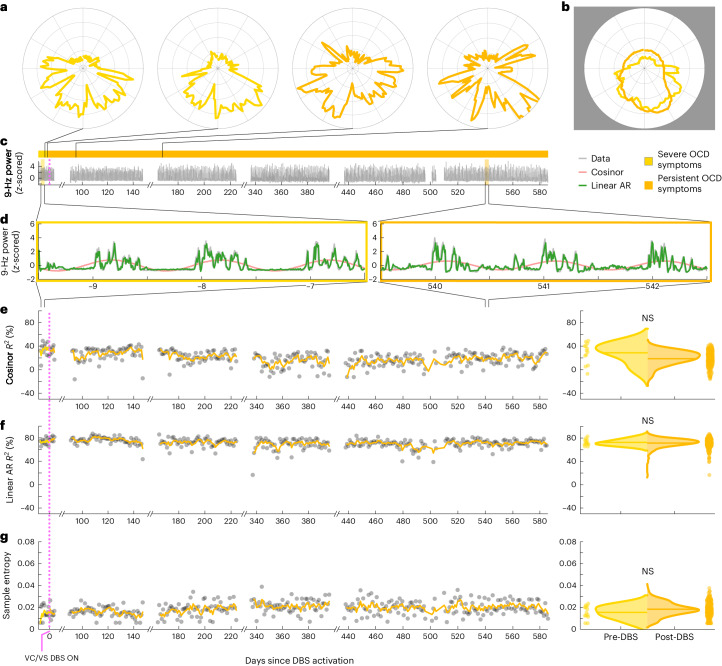
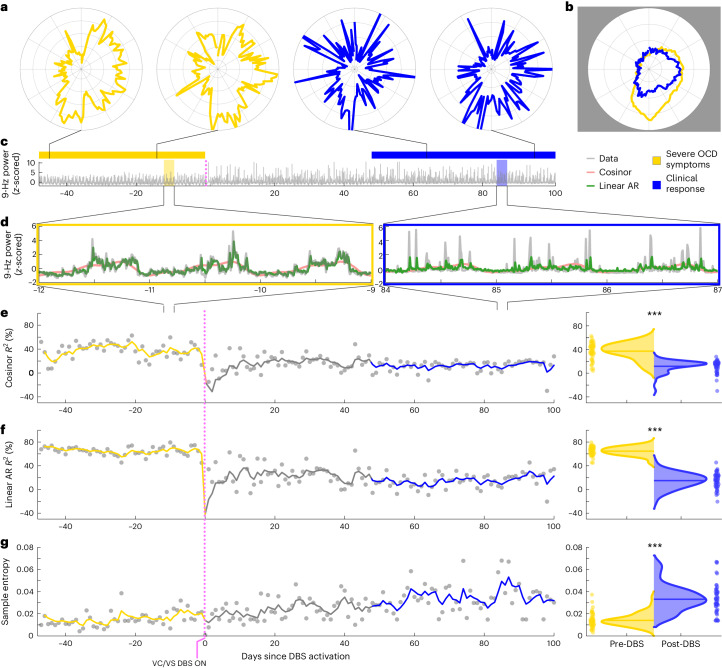
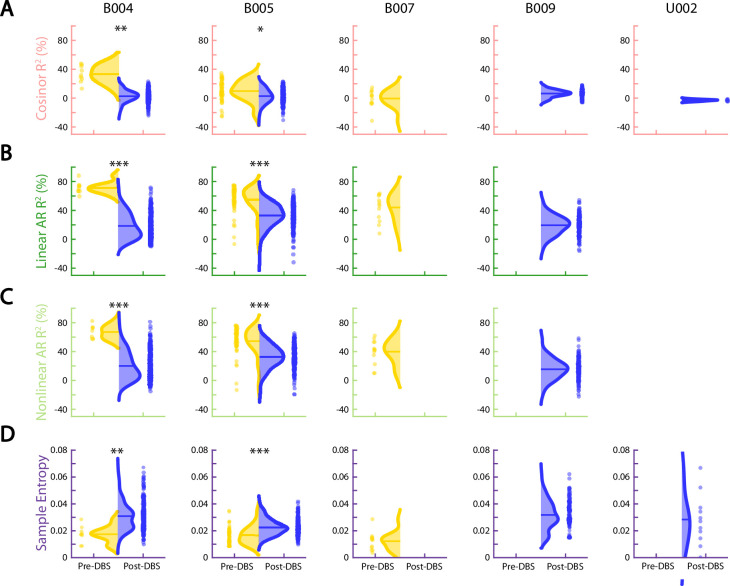
Recent advances in surgical neuromodulation have enabled chronic and continuous intracranial monitoring during everyday life. We used this opportunity to identify neural predictors of clinical state in 12 individuals with treatment-resistant obsessive-compulsive disorder (OCD) receiving deep brain stimulation (DBS) therapy ( NCT05915741 ). We developed our neurobehavioral models based on continuous neural recordings in the region of the ventral striatum in an initial cohort of five patients and tested and validated them in a held-out cohort of seven additional patients. Before DBS activation, in the most symptomatic state, theta/alpha (9 Hz) power evidenced a prominent circadian pattern and a high degree of predictability. In patients with persistent symptoms (non-responders), predictability of the neural data remained consistently high. On the other hand, in patients who improved symptomatically (responders), predictability of the neural data was significantly diminished. This neural feature accurately classified clinical status even in patients with limited duration recordings, indicating generalizability that could facilitate therapeutic decision-making.
© 2024. The Author(s).
Conflict of interest statement
S.A.S. has been a consultant for Boston Scientific, Zimmer Biomet, Koh Young, Sensoria Therapeutics, Varian Medical Systems, Abbott and Neuropace and is co-founder of Motif Neurotech. W.K.G. receives royalties from Nview, LLC and OCDscales, LLC. E.A.S. reports receiving research funding to his institution from the Ream Foundation, the International OCD Foundation and the National Institutes of Health. He was formerly a consultant for Brainsway and Biohaven Pharmaceuticals in the past 12 months. He owns stock less than $5,000 in NView/Proem for distribution related to the Y-BOCS scales. He receives book royalties from Elsevier, Wiley, Oxford, the American Psychological Association, Guildford, Springer, Routledge and Jessica Kingsley. A.B.P. has been an advisor to Endoluxe, CSDISCO and SCAN Health Plan and is co-founder and CEO of Audit AI. B.J.M. has received research support from LivaNova and Health Rhythms in the past 2 years. The other authors declare no competing interests.
Figures



References
-
- Insel, T. et al. Research domain criteria (RDoC): toward a new classification framework for research on mental disorders. Am. J. Psychiatry167, 748–751 (2010). - PubMed
-
- Mostofsky, S. H. & Simmonds, D. J. Response inhibition and response selection: two sides of the same coin. J. Cogn. Neurosci.20, 751–761 (2008). - PubMed
-
- Botvinick, M. M., Braver, T. S., Barch, D. M., Carter, C. S. & Cohen, J. D. Conflict monitoring and cognitive control. Psychol. Rev.108, 624–652 (2001). - PubMed
-
- Kahneman, D. Thinking, Fast and Slow (Macmillan, 2011).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
