

Trace of delirium after robotic lower abdominal tumor resection at different end-tidal carbon dioxide: a RCT trial
- PMID: 38997624
- PMCID: PMC11241950
- DOI: 10.1186/s12871-024-02617-3
Trace of delirium after robotic lower abdominal tumor resection at different end-tidal carbon dioxide: a RCT trial
Abstract
Background: Postoperative delirium (POD) often occurs in oncology patients, further increasing the medical and financial burden. Robotic technology in lower abdominal tumors resection reduces surgical trauma but increases risks such as carbon dioxide (CO2) absorption. This study aimed to investigate the differences in their occurrence of POD at different end-tidal CO2 levels.
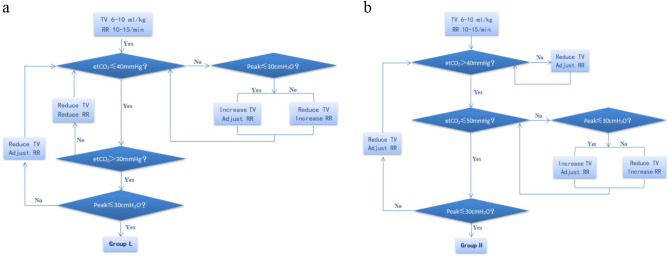
Method: This study was approved by the Ethics Committee of Affiliated Hospital of He Bei University (HDFY-LL-2022-169). The study was registered with the Chinese Clinical Trials Registry on URL: http://www.chictr.org.cn , Registry Number: ChiCTR2200056019 (Registry Date: 27/08/2022). In patients scheduled robotic lower abdominal tumor resection from September 1, 2022 to December 31, 2022, a comprehensive delirium assessment was performed three days postoperatively using the CAM scale with clinical review records. Intraoperative administration of different etCO2 was performed depending on the randomized grouping after intubation. Group L received lower level etCO2 management (31-40mmHg), and Group H maintained the higher level(41-50mmHg) during pneumoperitoneum. Data were analyzed using Pearson Chi-Square or Wilcoxon Rank Sum tests and multiple logistic regression. Preoperative mental status score, alcohol impairment score, nicotine dependence score, history of hypertension and diabetes, duration of surgery and worst pain score were included in the regression model along with basic patient information for covariate correction analysis.
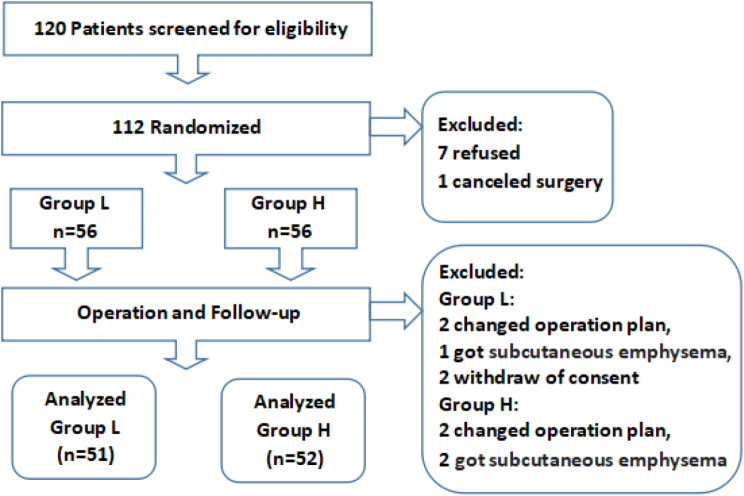
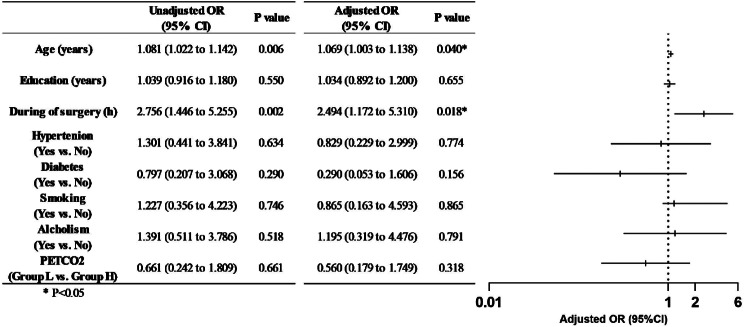
Results: Among the 103 enrolled patients, 19 (18.4%) developed postoperative delirium. The incidence of delirium in different etCO2 groups was 21.6% in Group L and 15.4% in Group H, respectively, with no statistical differences. In adjusted multivariate analysis, age and during of surgery were statistically significant predictors of postoperative delirium. The breath-hold test was significantly lower postoperatively, but no statistical differences were found between two groups.
Conclusion: With robotic assistant, the incidence of postoperative delirium in patients undergoing lower abdominal tumor resection was not modified by different end-tidal carbon dioxide management, however, age and duration of surgery were positively associated risk factors.
Keywords: End-tidal carbon dioxide; Postoperative delirium; Robotic surgery; Tumor resection.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Preoperative frailty tendency predicts delirium occurrence in older people undergoing spinal surgery.BMC Geriatr. 2024 Oct 22;24(1):856. doi: 10.1186/s12877-024-05476-2. BMC Geriatr. 2024. PMID: 39438819 Free PMC article.
-
Intraoperative Electroencephalogram Frontal Low Alpha Power for Predicting Postoperative Delirium in Elderly Patients after Orthopedic Surgery: A Prospective Cohort Study.Ann Ital Chir. 2024;95(6):1134-1146. doi: 10.62713/aic.3641. Ann Ital Chir. 2024. PMID: 39723508
-
Intraoperative Oxygen Concentration and Postoperative Delirium After Laparoscopic Gastric and Colorectal Malignancies Surgery: A Randomized, Double-Blind, Controlled Trial.Clin Interv Aging. 2021 Jun 15;16:1085-1093. doi: 10.2147/CIA.S311190. eCollection 2021. Clin Interv Aging. 2021. PMID: 34163152 Free PMC article. Clinical Trial.
-
Effect of different durations of preoperative computerised cognitive training on postoperative delirium in older patients undergoing cardiac surgery: a study protocol for a prospective, randomised controlled trial.BMJ Open. 2024 Nov 14;14(11):e088163. doi: 10.1136/bmjopen-2024-088163. BMJ Open. 2024. PMID: 39542468 Free PMC article.
-
The association between preoperative lacunar infarcts and postoperative delirium in elderly patients undergoing major abdominal surgery: a prospective cohort study.Aging Clin Exp Res. 2025 Jan 29;37(1):35. doi: 10.1007/s40520-024-02909-1. Aging Clin Exp Res. 2025. PMID: 39878919 Free PMC article. Review.
References
-
- World H, Orgnization. ICD-11 2022 release,. [Online]. Available: https://www.who.int/news/item/11-02-2022-icd-11-2022-release. Accessed: 2023/2/20.
-
- Adamis D, Meagher D, Rooney S, Mulligan O, McCarthy G. A comparison of outcomes according to different diagnostic systems for delirium (DSM-5, DSM-IV, CAM, and DRS-R98), Int. Psychogeriatr, vol. 30, no. 4, pp. 591–596, 2018 Apr 2018. 10.1017/S1041610217001697. - PubMed
-
- Wada S et al. Preoperative anxiety as a predictor of Delirium in Cancer patients: a prospective Observational Cohort Study. World J Surg, 43, 1, pp. 134–42, 2019 Jan 2019. 10.1007/s00268-018-4761-0. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
