

Differences of anticholinergic drug burden between older hospitalized patients with and without delirium: a systematic review and meta-analysis based on prospective cohort studies
- PMID: 38997670
- PMCID: PMC11241997
- DOI: 10.1186/s12877-024-05197-6
Differences of anticholinergic drug burden between older hospitalized patients with and without delirium: a systematic review and meta-analysis based on prospective cohort studies
Abstract
Objectives: This review aims to comprehensively summarize the differences in anticholinergic drug burden (ADB) scores between older hospitalized patients with and without delirium.
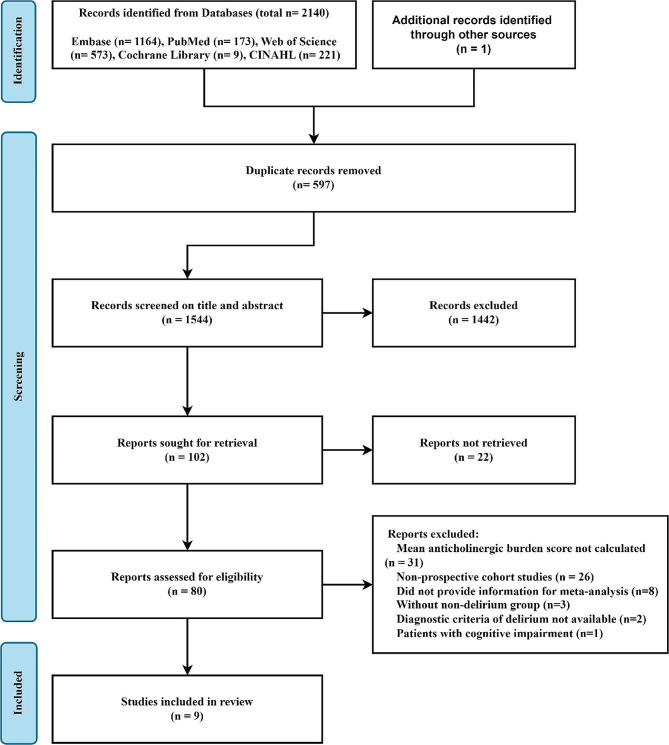
Methods: We searched PubMed, Embase, Web of Science, Cochrane Library and CINAHL EBSCOhost databases to identify prospective cohort studies exploring the relationship between ADB and the occurrence of delirium in older hospitalized patients. The primary outcome of the review was the mean ADB scores for the delirium and non-delirium groups, and the secondary outcome was the scores for the subsyndromal and non-delirium groups. The standardized mean difference (SMD) and corresponding 95% confidence intervals (95% CI) were incorporated using a fixed-effect method. Moreover, we performed subgroup analysis according to the admission type, age, the ADB scale type and the ADB classification.
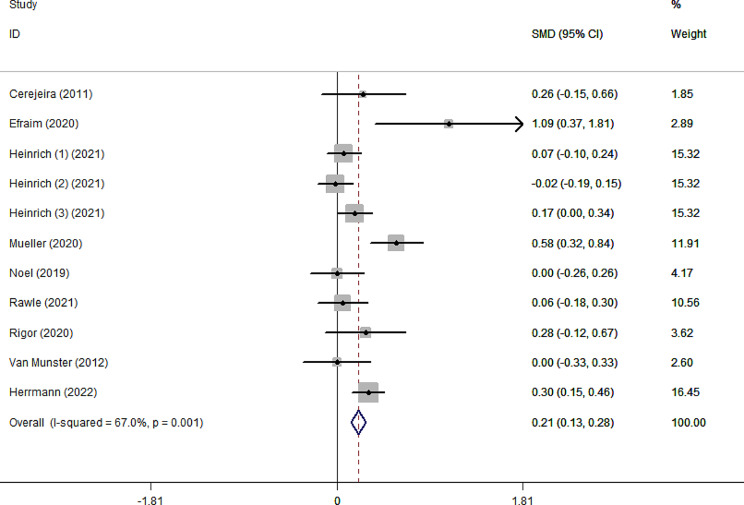
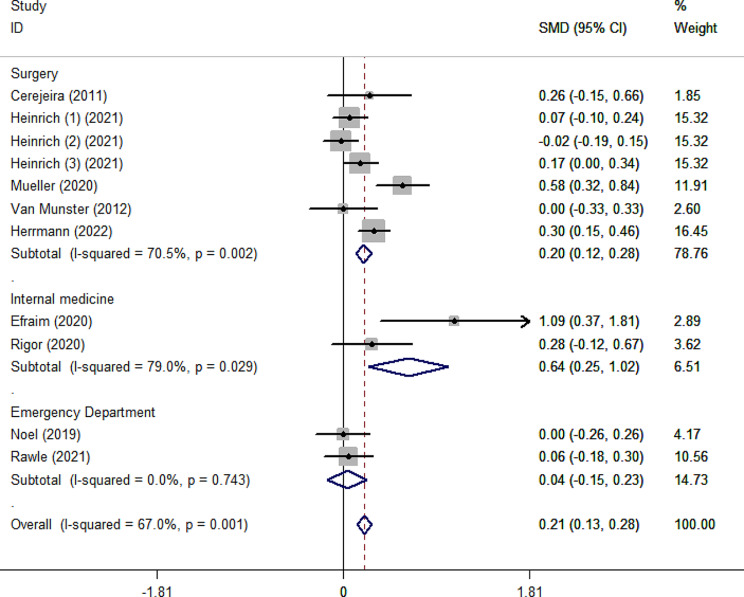
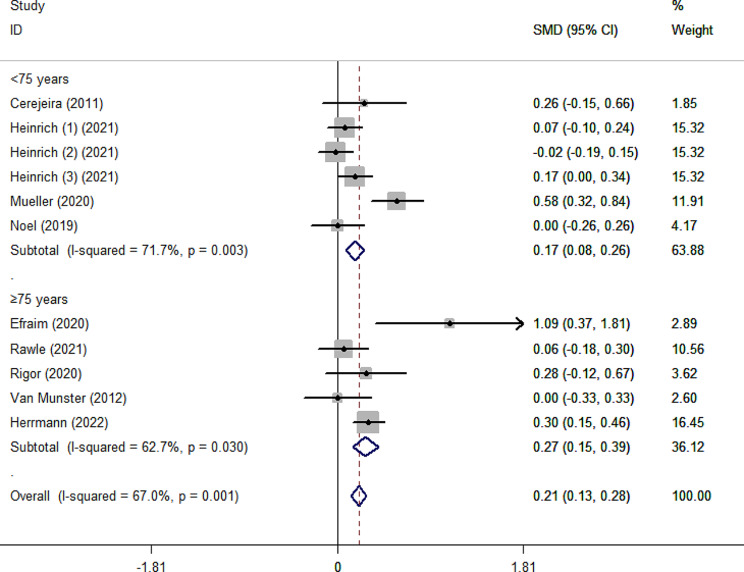
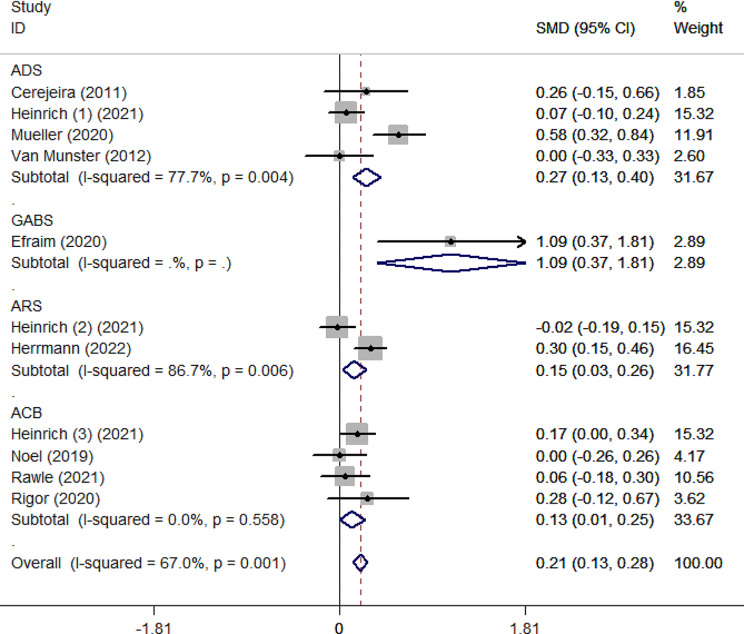
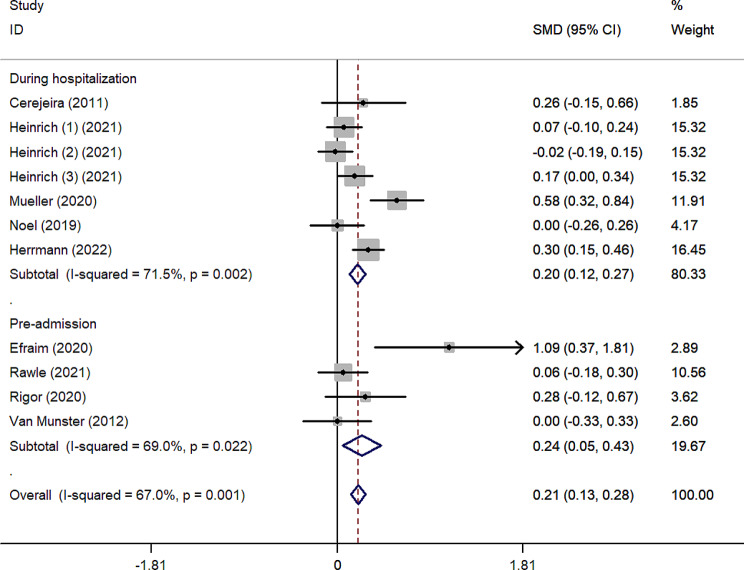
Results: Nine prospective cohort studies involving 3791 older patients with a median age of 75.1 (71.6-83.9) were included. The ADB score was significantly higher in the delirium group than in the non-delirium group (SMD = 0.21, 95%CI 0.13-0.28). In subgroup analysis, the age subgroup was split into < 75 and ≥ 75 according to the median age of the older people. There were significant differences in ADB scores between older people with delirium and those without delirium in various subgroups: surgical (SMD = 0.20, 95%CI 0.12-0.28), internal medicine (SMD = 0.64, 95%CI 0.25-1.02), age < 75 (SMD = 0.17, 95%CI 0.08-0.26), age ≥ 75 (SMD = 0.27, 95%CI 0.15-0.39), ADS scale (SMD = 0.13, 95%CI 0.13-0.40), ARS scale (SMD = 0.15, 95%CI 0.03-0.26), ACB scale (SMD = 0.13, 95%CI 0.01-0.25), pre-admission ADB (SMD = 0.24, 95%CI 0.05-0.43) and ADB during hospitalization (SMD = 0.20, 95%CI 0.12-0.27).
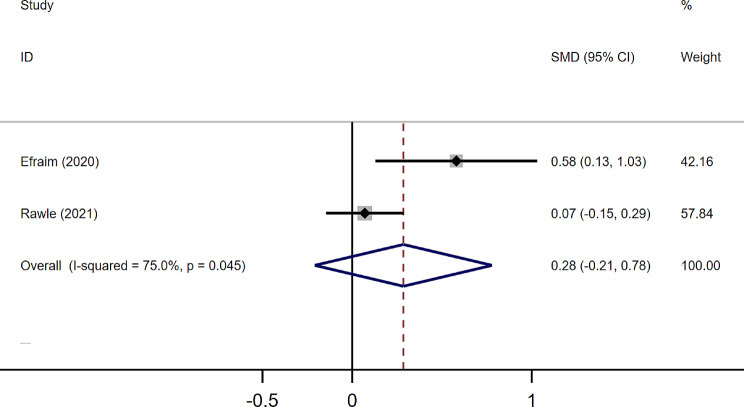
Conclusions: We found a quantitative relationship between ADB and delirium in older patients admitted for internal medicine and surgery. And this relationship remained significant in different age, ADB scale type and ADB classification subgroups. However, the actual difference in ADB scores between patients with delirium and without delirium was small. More high-quality observational studies should be conducted to explore the impact of ADB on delirium and subsyndromal delirium.
Clinical trial registration: The protocol was published in the International Prospective Register of Systematic Reviews (PROSPERO) [Ref: CRD42022353649].
Keywords: Anticholinergic drug burden; Delirium; Meta-analysis; Older hospitalized patients; Relationship.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Boustani M, Campbell N, Munger S, Maidment I, Fox C. Impact of anticholinergics on the aging brain: a review and practical application. Aging Health. 2008;4(3):311–20. doi: 10.2217/1745509X.4.3.311. - DOI
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
