

Traumatic Brain Injury as an Independent Predictor of Futility in the Early Resuscitation of Patients in Hemorrhagic Shock
- PMID: 38999481
- PMCID: PMC11242176
- DOI: 10.3390/jcm13133915
Traumatic Brain Injury as an Independent Predictor of Futility in the Early Resuscitation of Patients in Hemorrhagic Shock
Abstract
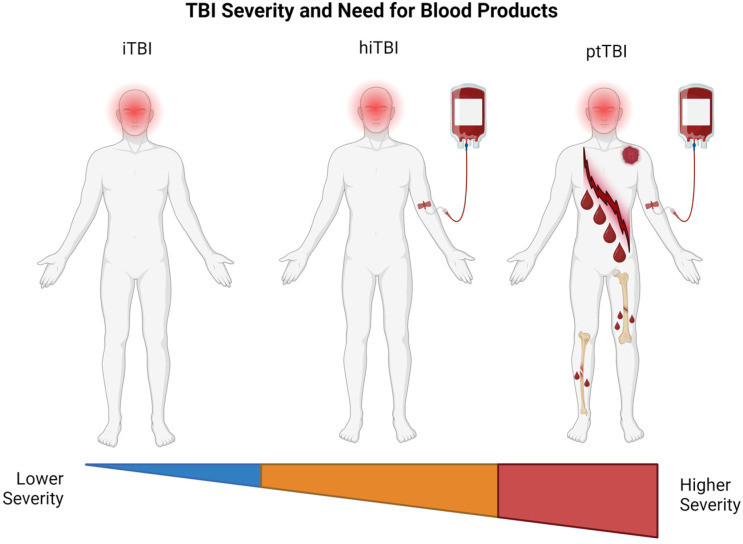
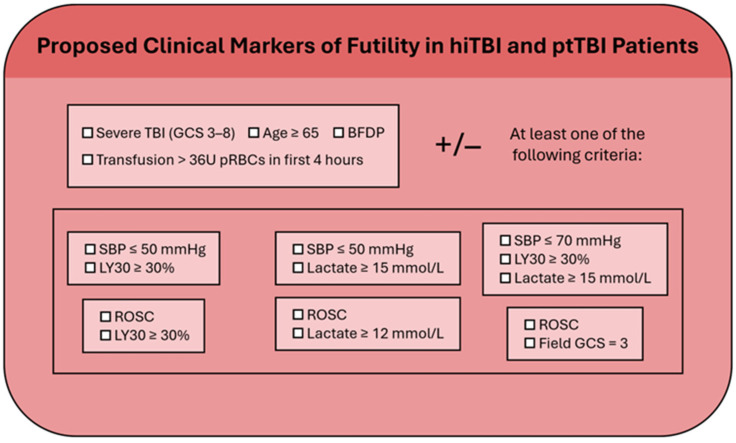
This review explores the concept of futility timeouts and the use of traumatic brain injury (TBI) as an independent predictor of the futility of resuscitation efforts in severely bleeding trauma patients. The national blood supply shortage has been exacerbated by the lingering influence of the COVID-19 pandemic on the number of blood donors available, as well as by the adoption of balanced hemostatic resuscitation protocols (such as the increasing use of 1:1:1 packed red blood cells, plasma, and platelets) with and without early whole blood resuscitation. This has underscored the urgent need for reliable predictors of futile resuscitation (FR). As a result, clinical, radiologic, and laboratory bedside markers have emerged which can accurately predict FR in patients with severe trauma-induced hemorrhage, such as the Suspension of Transfusion and Other Procedures (STOP) criteria. However, the STOP criteria do not include markers for TBI severity or transfusion cut points despite these patients requiring large quantities of blood components in the STOP criteria validation cohort. Yet, guidelines for neuroprognosticating patients with TBI can require up to 72 h, which makes them less useful in the minutes and hours following initial presentation. We examine the impact of TBI on bleeding trauma patients, with a focus on those with coagulopathies associated with TBI. This review categorizes TBI into isolated TBI (iTBI), hemorrhagic isolated TBI (hiTBI), and polytraumatic TBI (ptTBI). Through an analysis of bedside parameters (such as the proposed STOP criteria), coagulation assays, markers for TBI severity, and transfusion cut points as markers of futilty, we suggest amendments to current guidelines and the development of more precise algorithms that incorporate prognostic indicators of severe TBI as an independent parameter for the early prediction of FR so as to optimize blood product allocation.
Keywords: emergency; futility; hemorrhage; massive transfusion; resuscitation; shock; trauma; traumatic brain injury.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
