

Biochemical and Histological Differences between Longitudinal and Vertical Fibres of Dupuytren's Palmar Aponeurosis and Innovative Clinical Implications
- PMID: 38999972
- PMCID: PMC11241458
- DOI: 10.3390/ijms25136865
Biochemical and Histological Differences between Longitudinal and Vertical Fibres of Dupuytren's Palmar Aponeurosis and Innovative Clinical Implications
Abstract
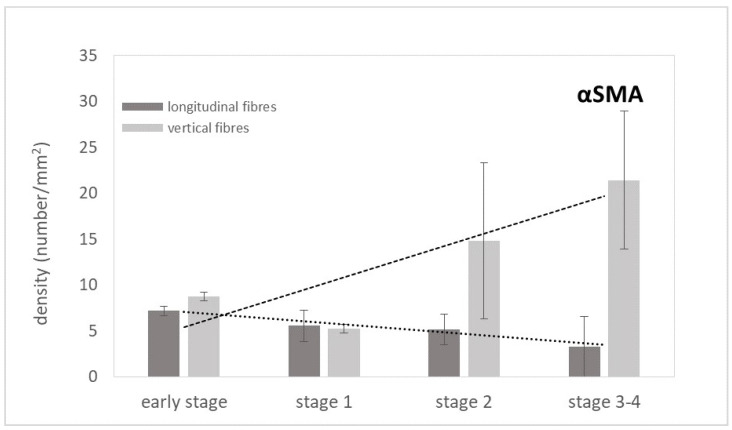
Dupuytren's disease, a chronic and progressive fibroproliferative lesion of the hand, which affects the palmar fascia, has a recurrence rate after selective aponeurotomy of 20-40% at 5 years. This study focused, for the first time, on the microanatomical and histopathological characteristics of the longitudinal and vertical fibres (usually spared during surgery) in the aponeurosis with Dupuytren's disease, in different stages of the Tubiana's classification. Twelve human samples were collected and analysed by immunostaining, Total Collagen Assay, ELISA Immunoassay, and immunoblotting for the Von Willebrand factor, α-Sma, D2-40, CD-68, Total Collagen, Collagen-I and III, IL1β, TNF-α to analyse the blood and lymphatic vascularization, the amount and distribution of collagen, and the inflammation. The results show a progressive increase in the arterial vascularization in the vertical fibres (from 8.8/mm2 in the early stage to 21.4/mm2 in stage 3/4), and a parallel progressive decrease in the lymphatic drainage (from 6.2/mm2 to 2.8/mm2), correlated with a local inflammatory context (increase in IL-1β and TNF-α until the stage 2) in both the longitudinal and vertical fibres. The acute inflammation after stage 2 decreased, in favour of a fibrotic action, with the clear synthesis of new collagen (up to ~83 µg/mg), especially Collagen-I. These results clearly demonstrate the involvement of the septa of Legueu and Juvara in the disease pathology and the modifications with the disease's progression. A greater understanding of the pathology becomes fundamental for staging and the adequate therapeutic timing, to obtain the best morpho-functional result and the lowest risk of complications.
Keywords: Dupuytren’s disease; collagen; fibrosis; inflammation; palmar fascia.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures












Similar articles
-
Dupuytren's contracture: morphological and biochemical changes in palmar aponeurosis.Hand. 1982 Oct;14(3):237-47. doi: 10.1016/s0072-968x(82)80056-9. Hand. 1982. PMID: 6130030
-
Dupuytren's cord involving the septa of Legueu and Juvara: a case report.J Hand Surg Am. 2002 Mar;27(2):344-6. doi: 10.1053/jhsu.2002.32080. J Hand Surg Am. 2002. PMID: 11901396
-
Active synthesis of type I collagen homotrimer in Dupuytren's fibrosis is unaffected by anti-TNF-α treatment.JCI Insight. 2025 May 8;10(9):e175188. doi: 10.1172/jci.insight.175188. eCollection 2025 May 8. JCI Insight. 2025. PMID: 40337865 Free PMC article.
-
[The fibrous skeleton of the hand : Changes with Dupuytren's contracture].Orthopade. 2017 Apr;46(4):303-314. doi: 10.1007/s00132-017-3406-6. Orthopade. 2017. PMID: 28361190 German.
-
Palmar fascial complex anatomy and pathology in Dupuytren's disease.Hand Clin. 1999 Feb;15(1):73-86, vi-vii. Hand Clin. 1999. PMID: 10050244 Review.
Cited by
-
The Impact of Sciatic Nerve Injury on Extracellular Matrix of Lower Limb Muscle and Thoracolumbar Fascia: An Observational Study.Int J Mol Sci. 2024 Aug 16;25(16):8945. doi: 10.3390/ijms25168945. Int J Mol Sci. 2024. PMID: 39201630 Free PMC article.
-
Pathological Changes in Extracellular Matrix Composition Orchestrate the Fibrotic Feedback Loop Through Macrophage Activation in Dupuytren's Contracture.Int J Mol Sci. 2025 Mar 28;26(7):3146. doi: 10.3390/ijms26073146. Int J Mol Sci. 2025. PMID: 40243889 Free PMC article.
References
-
- Warwick D., editor. Dupuytren’s Disease. FESSH Instructional Course. C. G. Edizioni Medico Scientifiche; Torino, Italy: 2015.
-
- Tubiana R., Leclercq C., Hurst L.C., Badalamente M.A., Mackin E.J. Dupuytren’s Disease. Martin Dunitz Ltd.; London, UK: 2000.
-
- Karkampouna S., Kreulen M., Obdeijn M.C., Kloen P., Dorjée A.L., Rivellese F., Chojnowski A., Clark I., Kruithof-de Julio M. Connective Tissue Degeneration: Mechanisms of Palmar Fascia Degeneration (Dupuytren’s Disease) Curr. Mol. Biol. Rep. 2016;2:133–140. doi: 10.1007/s40610-016-0045-3. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
