

New Insights into Hepatic and Intestinal Microcirculation and Pulmonary Inflammation in a Model of Septic Shock and Veno-Arterial Extracorporeal Membrane Oxygenation in the Rat
- PMID: 39000529
- PMCID: PMC11242878
- DOI: 10.3390/ijms25137421
New Insights into Hepatic and Intestinal Microcirculation and Pulmonary Inflammation in a Model of Septic Shock and Veno-Arterial Extracorporeal Membrane Oxygenation in the Rat
Abstract
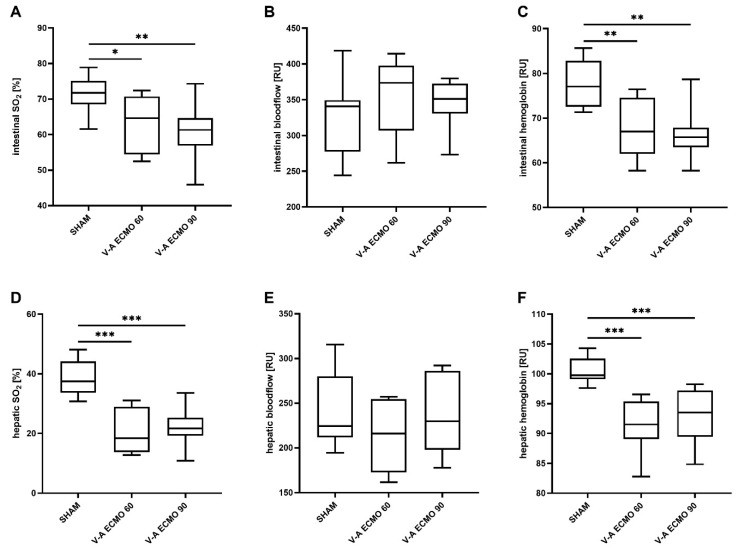
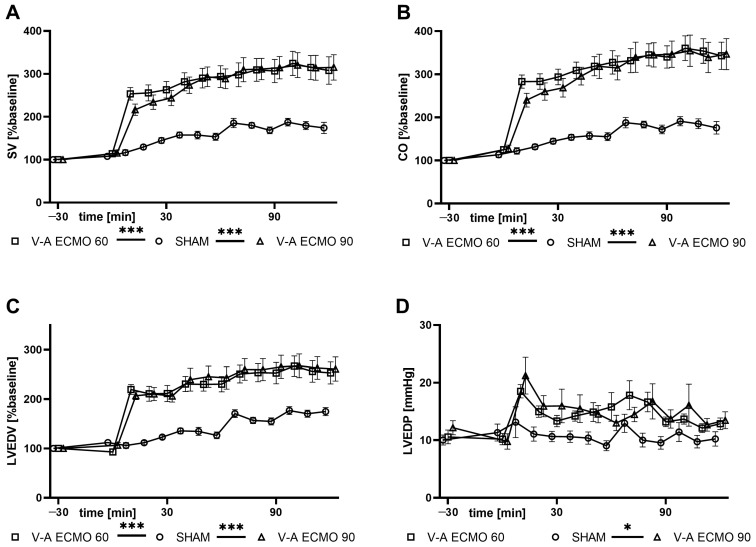
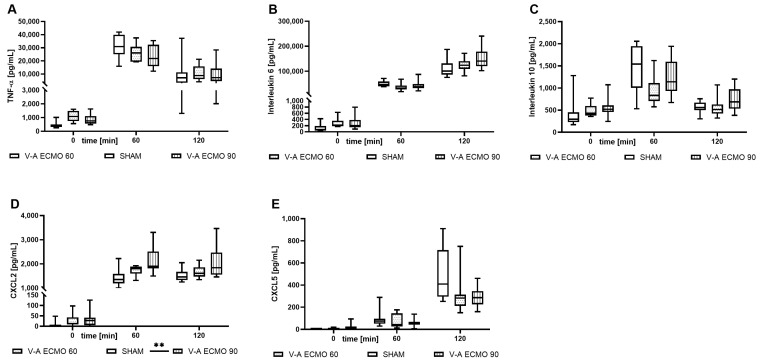
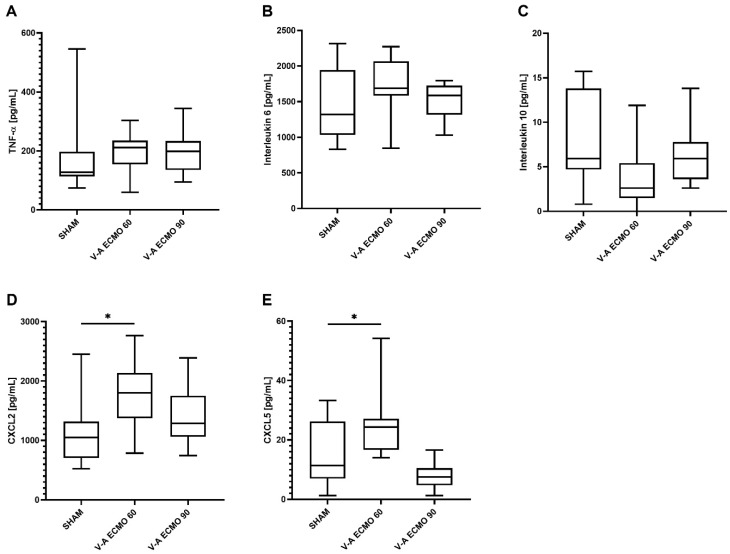
Despite significant efforts toward improving therapy for septic shock, mortality remains high. Applying veno-arterial (V-A) extracorporeal membrane oxygenation (ECMO) in this context remains controversial. Since the cannulation of the femoral artery for V-A ECMO return leads to lower body hyperoxia, this study investigated the impact of V-A ECMO therapy on the intestinal and hepatic microcirculation during septic shock in a rodent model. Thirty male Lewis rats were randomly assigned to receive V-A ECMO therapy with low (60 mL/kg/min) or high (90 mL/kg/min) blood flow or a sham procedure. Hemodynamic data were collected through a pressure-volume catheter in the left ventricle and a catheter in the lateral tail artery. Septic shock was induced by intravenous administration of lipopolysaccharide (1 mg/kg). The rats received lung-protective ventilation during V-A ECMO therapy. The hepatic and intestinal microcirculation was measured by micro-lightguide spectrophotometry after median laparotomy for two hours. Systemic and pulmonary inflammation was detected via enzyme-linked immunosorbent assays (ELISA) of the plasma and bronchoalveolar lavage (BAL), respectively, measuring tumor necrosis factor-alpha (TNF-α), interleukins 6 (IL-6) and 10 (IL-10), and C-X-C motif ligands 2 (CXCL2) and 5 (CXCL5). Oxygen saturation and relative hemoglobin concentration were reduced in the hepatic and intestinal microcirculation during V-A ECMO therapy, independent of the blood flow rate. Further, rats treated with V-A ECMO therapy also presented elevated systolic, diastolic, and mean arterial blood pressure and increased stroke volume, cardiac output, and left ventricular end-diastolic volume. However, left ventricular end-diastolic pressure was only elevated during high-flow V-A ECMO therapy. Blood gas analysis revealed a dilutional anemia during V-A ECMO therapy. ELISA analysis showed an elevated plasma CXCL2 concentration only during high-flow V-A ECMO therapy and elevated BAL CXCL2 and CXCL5 concentrations only during low-flow V-A ECMO therapy. Rats undergoing V-A ECMO therapy exhibited impaired microcirculation of the intestine and liver during septic shock despite increased blood pressure and cardiac output. Increased pulmonary inflammation was detected only during low-flow V-A ECMO therapy in septic shock.
Keywords: V-A ECMO; inflammation; intestinal perfusion; sepsis.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures

Similar articles
-
New Insights into Hepatic and Intestinal Microcirculation and Pulmonary Inflammation in a Model of Septic Shock and Venovenous Extracorporeal Membrane Oxygenation in the Rat.Int J Mol Sci. 2024 Jun 16;25(12):6621. doi: 10.3390/ijms25126621. Int J Mol Sci. 2024. PMID: 38928327 Free PMC article.
-
Micro-lightguide spectrophotometry assessment of hepatic and intestinal microcirculation in endotoxemic rats during intravenous treatment with angiotensin II.Eur J Pharm Sci. 2023 Dec 1;191:106588. doi: 10.1016/j.ejps.2023.106588. Epub 2023 Sep 20. Eur J Pharm Sci. 2023. PMID: 37734468
-
Effect of increased cardiac output on hepatic and intestinal microcirculatory blood flow, oxygenation, and metabolism in hyperdynamic murine septic shock.Crit Care Med. 2005 Oct;33(10):2332-8. doi: 10.1097/01.ccm.0000182817.20977.e9. Crit Care Med. 2005. PMID: 16215389
-
Venoarterial extracorporeal membrane oxygenation as mechanical circulatory support in adult septic shock: a systematic review and meta-analysis with individual participant data meta-regression analysis.Crit Care. 2021 Jul 14;25(1):246. doi: 10.1186/s13054-021-03668-5. Crit Care. 2021. PMID: 34261492 Free PMC article.
-
Extracorporeal Membrane Oxygenation for Septic Shock in Adults and Children: A Narrative Review.J Clin Med. 2023 Oct 20;12(20):6661. doi: 10.3390/jcm12206661. J Clin Med. 2023. PMID: 37892799 Free PMC article. Review.
Cited by
-
Extracorporeal membrane oxygenation vs cardiopulmonary bypass in lung transplantation: an updated meta-analysis.Gen Thorac Cardiovasc Surg. 2025 Mar;73(3):137-146. doi: 10.1007/s11748-024-02114-x. Epub 2024 Dec 21. Gen Thorac Cardiovasc Surg. 2025. PMID: 39708283
References
-
- Fleischmann-Struzek C., Mellhammar L., Rose N., Cassini A., Rudd K.E., Schlattmann P., Allegranzi B., Reinhart K. Incidence and mortality of hospital- and ICU-treated sepsis: Results from an updated and expanded systematic review and meta-analysis. Intensive Care Med. 2020;46:1552–1562. doi: 10.1007/s00134-020-06151-x. - DOI - PMC - PubMed
-
- Singer M., Deutschman C.S., Seymour C.W., Shankar-Hari M., Annane D., Bauer M., Bellomo R., Bernard G.R., Chiche J.-D., Coopersmith C.M., et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) JAMA. 2016;315:801–810. doi: 10.1001/jama.2016.0287. - DOI - PMC - PubMed
-
- Evans L., Rhodes A., Alhazzani W., Antonelli M., Coopersmith C.M., French C., Machado F.R., Mcintyre L., Ostermann M., Prescott H.C., et al. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021;47:1181–1247. doi: 10.1007/s00134-021-06506-y. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
