

Head-to-Head Comparison: P-POSSUM and ACS-NSQIP® in Predicting Perioperative Risk in Robotic Surgery for Gynaecological Cancers
- PMID: 39001360
- PMCID: PMC11240461
- DOI: 10.3390/cancers16132297
Head-to-Head Comparison: P-POSSUM and ACS-NSQIP® in Predicting Perioperative Risk in Robotic Surgery for Gynaecological Cancers
Abstract
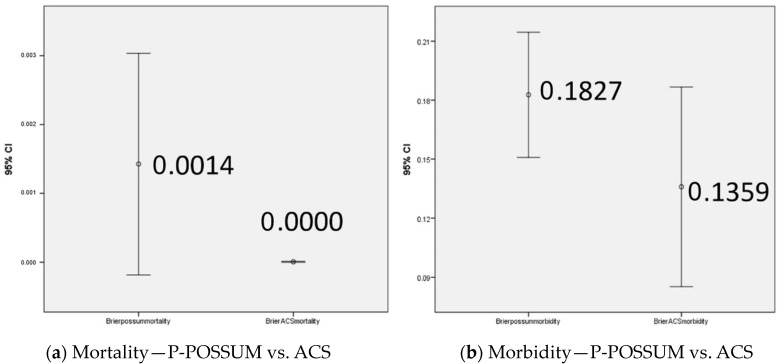
Purpose: In this retrospective pilot study, we aim to evaluate the accuracy and reliability of the P-POSSUM and ACS-NSQIP surgical risk calculators in predicting postoperative complications in gynaecological-oncological (GO) robotic surgery (RS). Methods: Retrospective data collection undertaken through a dedicated GO database and patient notes at a tertiary referral cancer centre. Following data lock with the actual post-op event/complication, the risk calculators were used to measure predictive scores for each patient. Baseline analysis of 153 patients, based on statistician advice, was undertaken to evaluate P-POSSUM and ACS-NSQIP validity and relevance in GO patients undergoing RS performed. Results: P-POSSUM reports on mortality and morbidity only; ACS-NSQIP reports some individual complications as well. ACS-NSQIP risk prediction was most accurate for venous thromboembolism (VTE) (area under the curve (AUC)-0.793) and pneumonia (AUC-0.657) and it showed 90% accuracy in prediction of five major complications (Brier score 0.01). Morbidity was much better predicted by ACS-NSQIP than by P-POSSUM (AUC-0.608 vs. AUC-0.551) with the same result in mortality prediction (Brier score 0.0000). Moreover, a statistically significant overestimation of morbidity has been shown by the P-POSSUM calculator (p = 0.018). Conclusions: Despite the limitations of this pilot study, the ACS-NSQIP risk calculator appears to be a better predictor of major complications and mortality, making it suitable for use by GO surgeons as an informed consent tool. Larger data collection and analyses are ongoing to validate this further.
Keywords: ACS-NSQIP; P-POSSUM; gynaecological oncology; morbidity; mortality; preoperative; risk prediction.
Conflict of interest statement
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures



References
-
- Kinnersley P., Phillips K., Savage K., Kelly M.J., Farrell E., Morgan B., Whistance R., Lewis V., Mann M.K., Stephens B.L., et al. Interventions to promote informed consent for patients undergoing surgical and other invasive healthcare procedures. Cochrane Database Syst. Rev. 2013;2013:1–247. doi: 10.1002/14651858.CD009445.PUB2. - DOI - PMC - PubMed
-
- Bowling A., Rowe G., Lambert N., Waddington M., Mahtani K., Kenten C., Howe A., Francis S. The measurement of patients’ expectations for health care: A review and psychometric testing of a measure of patients’ expectations. Health Technol. Assess. 2012;16:1–515. doi: 10.3310/HTA16300. - DOI - PubMed
-
- Stacey D., Légaré F., Col N.F., Bennett C.L., Barry M.J., Eden K.B., Holmes-Rovner M., Llewellyn-Thomas H., Lyddiatt A., Thomson R., et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst. Rev. 2014;2014:CD001431. doi: 10.1002/14651858.CD001431.PUB4. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
