

Evolving Precision First-Line Systemic Treatment for Patients with Unresectable Non-Small Cell Lung Cancer
- PMID: 39001412
- PMCID: PMC11240640
- DOI: 10.3390/cancers16132350
Evolving Precision First-Line Systemic Treatment for Patients with Unresectable Non-Small Cell Lung Cancer
Abstract
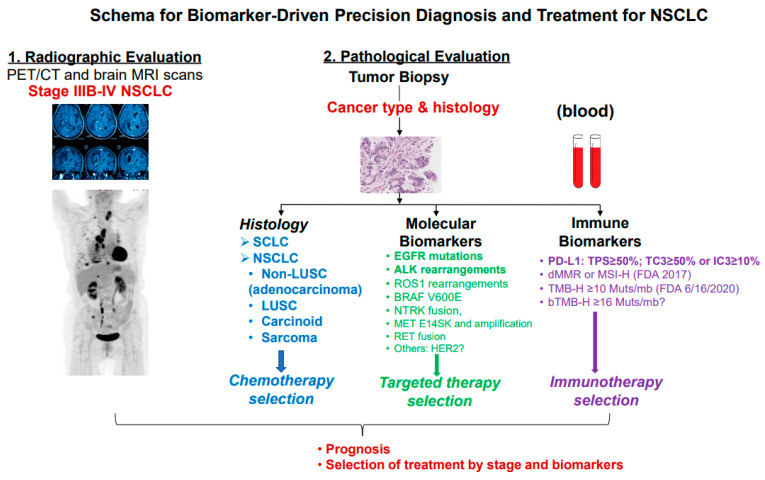
First-line systemic therapy for patients with advanced or metastatic non-small cell lung cancer (NSCLC) has rapidly evolved over the past two decades. First, molecularly targeted therapy for a growing number of gain-of-function molecular targets has been shown to improve progression-free survival (PFS) and overall survival (OS) with favorable toxicity profiles compared to platinum-containing chemotherapy and can be given as first-line systemic therapy in ~25% of patients with NSCLC. Actionable genetic alterations include EGFR, BRAF V600E, and MET exon 14 splicing site-sensitizing mutations, as well as ALK-, ROS1-, RET-, and NTRK-gene fusions. Secondly, inhibitors of programmed cell death protein 1 or its ligand 1 (PD-1/L1) such as pembrolizumab, atezolizumab, or cemiplimab monotherapy have become a standard of care for ~25% of patients with NSCLC whose tumors have high PD-L1 expression (total proportion score (TPS) ≥50%) and no sensitizing EGFR/ALK alterations. Lastly, for the remaining ~50% of patients who are fit and whose tumors have no or low PD-L1 expression (TPS of 0-49%) and no sensitizing EGFR/ALK aberrations, platinum-containing chemotherapy with the addition of a PD-1/L1 inhibitor alone or in combination of a cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) inhibitor improves PFS and OS compared to chemotherapy alone. The objectives of this review are to summarize the current data and perspectives on first-line systemic treatment in patients with unresectable NSCLC and propose a practical algorithm for implementing precision biomarker testing at diagnosis.
Keywords: CTLA-4; NSCLC; PD-1; PD-L1; biomarkers; first-line therapy; immune biomarkers; immune checkpoint inhibitors; molecular targets.
Conflict of interest statement
T.L. receives research grants to conduct clinical trials as principal investigator at local institute from AbbVie Inc., Astellas, AstraZeneca, BioNTech, Chugai Pharma, Duality Biologics, Genentech/LaRoche, Jounce Therapeutics, LabyRx Immuno-Oncology, Merck, OncoC4, Novartis, RasCal Therapeutics, Tempus, and Xilio Therapeutics.
Figures


Similar articles
-
Systemic treatments for metastatic cutaneous melanoma.Cochrane Database Syst Rev. 2018 Feb 6;2(2):CD011123. doi: 10.1002/14651858.CD011123.pub2. Cochrane Database Syst Rev. 2018. PMID: 29405038 Free PMC article.
-
Driving Best Practices Throughout the Treatment Journey for Patients with NSCLC with Actionable Alterations: A Podcast Discussion.Adv Ther. 2025 Aug;42(8):3591-3605. doi: 10.1007/s12325-025-03195-7. Epub 2025 May 22. Adv Ther. 2025. PMID: 40402375 Free PMC article.
-
Immune checkpoint inhibitors plus platinum-based chemotherapy compared to platinum-based chemotherapy with or without bevacizumab for first-line treatment of older people with advanced non-small cell lung cancer.Cochrane Database Syst Rev. 2024 Aug 13;8(8):CD015495. doi: 10.1002/14651858.CD015495. Cochrane Database Syst Rev. 2024. PMID: 39136258 Free PMC article.
-
Targeted therapy for advanced anaplastic lymphoma kinase (<I>ALK</I>)-rearranged non-small cell lung cancer.Cochrane Database Syst Rev. 2022 Jan 7;1(1):CD013453. doi: 10.1002/14651858.CD013453.pub2. Cochrane Database Syst Rev. 2022. PMID: 34994987 Free PMC article.
-
Efficacy and safety of immune checkpoint inhibitors for advanced non-small cell lung cancer with or without PD-L1 selection: A systematic review and network meta-analysis.Chin Med J (Engl). 2023 Sep 20;136(18):2156-2165. doi: 10.1097/CM9.0000000000002750. Epub 2023 Aug 18. Chin Med J (Engl). 2023. PMID: 37596898 Free PMC article.
Cited by
-
Preclinical Models for Functional Precision Lung Cancer Research.Cancers (Basel). 2024 Dec 25;17(1):22. doi: 10.3390/cancers17010022. Cancers (Basel). 2024. PMID: 39796653 Free PMC article. Review.
-
Prognostic role and functional impact of cadherin genes in non-small cell lung cancer tumorigenesis: mechanistic insights from in silico and in vitro analyses.PeerJ. 2025 Aug 19;13:e19785. doi: 10.7717/peerj.19785. eCollection 2025. PeerJ. 2025. PMID: 40860670 Free PMC article.
-
Clinical TNM Lung Cancer Staging: A Diagnostic Algorithm with a Pictorial Review.Diagnostics (Basel). 2025 Apr 1;15(7):908. doi: 10.3390/diagnostics15070908. Diagnostics (Basel). 2025. PMID: 40218258 Free PMC article. Review.
-
Recent Advances in PET and Radioligand Therapy for Lung Cancer: FDG and FAP.Cancers (Basel). 2025 Aug 1;17(15):2549. doi: 10.3390/cancers17152549. Cancers (Basel). 2025. PMID: 40805245 Free PMC article. Review.
-
Optimizing management of stage IV EGFR mutant non-small cell lung cancer in Asia: An expert opinion.Int J Cancer. 2025 Oct 15;157(8):1648-1661. doi: 10.1002/ijc.35512. Epub 2025 Jun 14. Int J Cancer. 2025. PMID: 40515576 Free PMC article.
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
