

The Current Position of Postoperative Radiotherapy for Salivary Gland Cancer: A Systematic Review and Meta-Analysis
- PMID: 39001437
- PMCID: PMC11240508
- DOI: 10.3390/cancers16132375
The Current Position of Postoperative Radiotherapy for Salivary Gland Cancer: A Systematic Review and Meta-Analysis
Abstract
Background: Because of the rarity, heterogeneous histology, and diverse anatomical sites of salivary gland cancer (SGC), there are a limited number of clinical studies on its management. This study reports the cumulative evidence of postoperative radiotherapy (PORT) for SGC of the head and neck.
Methods: A systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. We searched the PubMed, Embase, Cochrane Library, and Web of Science databases between 7th and 10th November 2023.
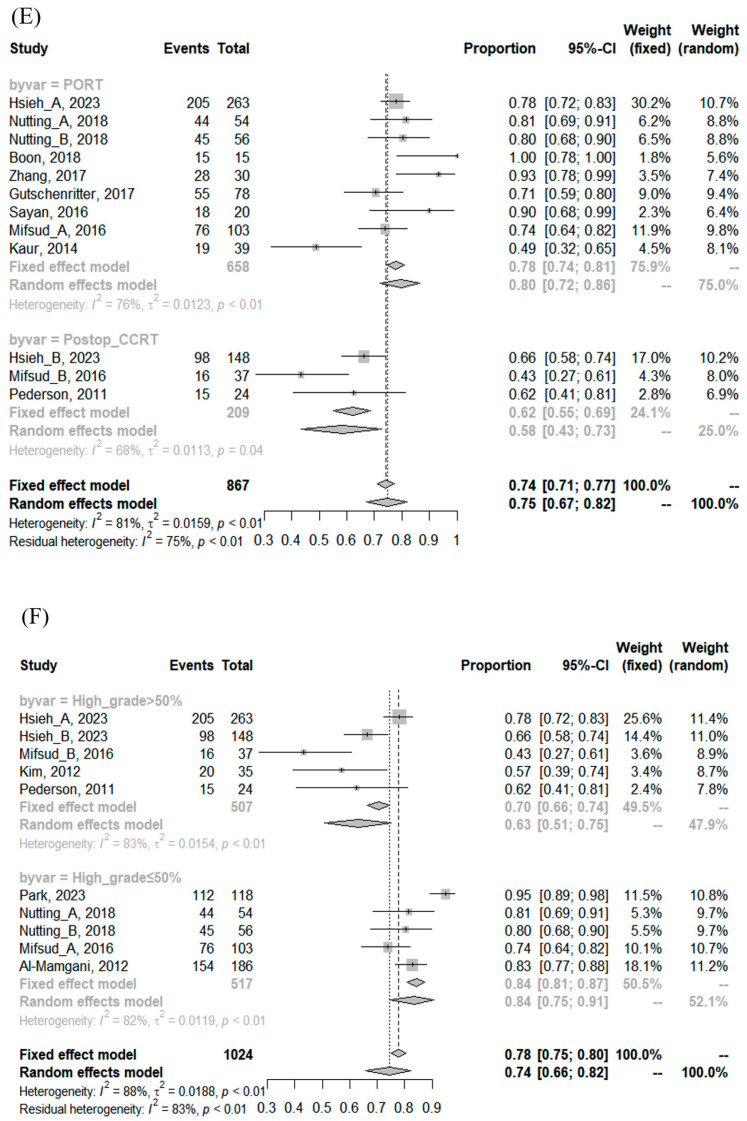
Results: A total of 2962 patients from 26 studies between 2007 and 2023 were included in this meta-analysis. The median RT dose was 64 Gy (range: 56-66 Gy). The median proportions of high-grade, pathological tumor stage 3 or 4 and pathological lymph node involvement were 42% (0-100%), 40% (0-77%), and 31% (0-75%). The pooled locoregional control rates at 3, 5, and 10 years were 92% (95% confidence interval [CI], 89-94%), 89% (95% CI, 86-93%), and 84% (95% CI, 73-92%), respectively. The pooled disease-free survival (DFS) rates at 3, 5, and 10 years were 77% (95% CI, 70-83%), 67% (95% CI, 60-74%), and 61% (95% CI, 55-67%), respectively. The pooled overall survival rates at 3, 5, and 10 years were 84% (95% CI, 79-88%), 75% (95% CI, 72-79%), and 68% (95% CI, 62-74%), respectively. Severe late toxicity ≥ grade 3 occurred in 7% (95% CI, 3-14%).
Conclusion: PORT showed favorable long-term efficacy and safety in SGC, especially for patients with high-grade histology. Considering that DFS continued to decrease, further clinical trials exploring treatment intensification are warranted.
Keywords: postoperative radiotherapy; radiotherapy; salivary gland cancer.
Conflict of interest statement
There are no conflicts of interest to declare.
Figures



Similar articles
-
Prognostic role of PD-L1 expression in patients with salivary gland carcinoma: A systematic review and meta-analysis.PLoS One. 2022 Jul 26;17(7):e0272080. doi: 10.1371/journal.pone.0272080. eCollection 2022. PLoS One. 2022. PMID: 35881656 Free PMC article.
-
Salivary gland carcinoma (SGC) with perineural spread and/or positive resection margin - high locoregional control rates after photon (chemo) radiotherapy - experience from a monocentric analysis.Radiat Oncol. 2019 Apr 23;14(1):68. doi: 10.1186/s13014-019-1260-x. Radiat Oncol. 2019. PMID: 31014362 Free PMC article.
-
The Current Evidence of Intensity-Modulated Radiotherapy for Hepatocellular Carcinoma: A Systematic Review and Meta-Analysis.Cancers (Basel). 2023 Oct 10;15(20):4914. doi: 10.3390/cancers15204914. Cancers (Basel). 2023. PMID: 37894281 Free PMC article. Review.
-
Safety and Survival Rates Associated With Ablative Stereotactic Radiotherapy for Patients With Oligometastatic Cancer: A Systematic Review and Meta-analysis.JAMA Oncol. 2021 Jan 1;7(1):92-106. doi: 10.1001/jamaoncol.2020.6146. JAMA Oncol. 2021. PMID: 33237270 Free PMC article.
-
Exploring All Avenues for Radiotherapy in Oligorecurrent Prostate Cancer Disease Limited to Lymph Nodes: A Systematic Review of the Role of Stereotactic Body Radiotherapy.Eur Urol Focus. 2017 Dec;3(6):538-544. doi: 10.1016/j.euf.2017.07.006. Epub 2017 Aug 8. Eur Urol Focus. 2017. PMID: 28801240
References
-
- Young A., Okuyemi O.T. Statpearls. StatPearls Publishing; Treasure Island, FL, USA: 2023. Malignant Salivary Gland Tumors. - PubMed
-
- Dos Santos E.S., Rodrigues-Fernandes C.I., Speight P.M., Khurram S.A., Alsanie I., Normando A.G.C., Prado-Ribeiro A.C., Brandao T.B., Kowalski L.P., Guerra E.N.S., et al. Impact of Tumor Site on the Prognosis of Salivary Gland Neoplasms: A Systematic Review and Meta-Analysis. Crit. Rev. Oncol. Hematol. 2021;162:103352. doi: 10.1016/j.critrevonc.2021.103352. - DOI - PubMed
-
- Thomson D.J., Slevin N.J., Mendenhall W.M. Indications for Salivary Gland Radiotherapy. Adv. Otorhinolaryngol. 2016;78:141–147. - PubMed
-
- Spiro R.H. Management of Malignant Tumors of the Salivary Glands. Oncology. 1998;12:671–680. Discussion 683. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
