

Transcript Markers from Urinary Extracellular Vesicles for Predicting Risk Reclassification of Prostate Cancer Patients on Active Surveillance
- PMID: 39001515
- PMCID: PMC11240337
- DOI: 10.3390/cancers16132453
Transcript Markers from Urinary Extracellular Vesicles for Predicting Risk Reclassification of Prostate Cancer Patients on Active Surveillance
Abstract
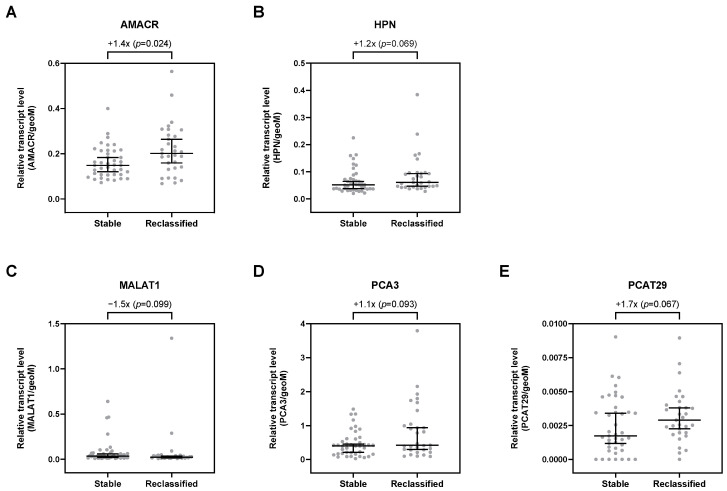
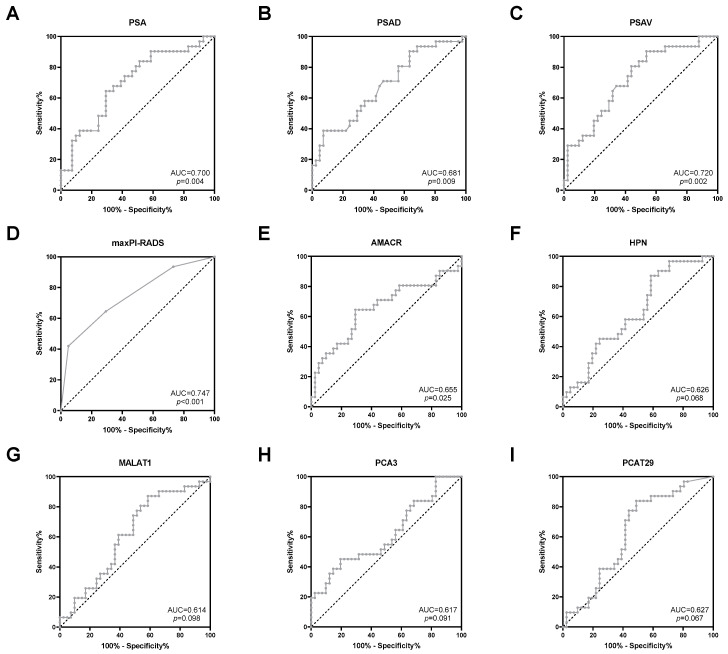
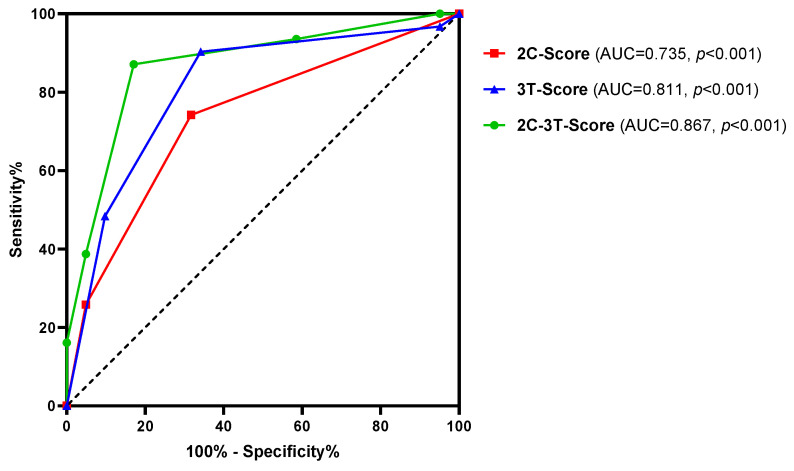
Serum prostate-specific antigen (PSA), its derivatives, and magnetic resonance tomography (MRI) lack sufficient specificity and sensitivity for the prediction of risk reclassification of prostate cancer (PCa) patients on active surveillance (AS). We investigated selected transcripts in urinary extracellular vesicles (uEV) from PCa patients on AS to predict PCa risk reclassification (defined by ISUP 1 with PSA > 10 ng/mL or ISUP 2-5 with any PSA level) in control biopsy. Before the control biopsy, urine samples were prospectively collected from 72 patients, of whom 43% were reclassified during AS. Following RNA isolation from uEV, multiplexed reverse transcription, and pre-amplification, 29 PCa-associated transcripts were quantified by quantitative PCR. The predictive ability of the transcripts to indicate PCa risk reclassification was assessed by receiver operating characteristic (ROC) curve analyses via calculation of the area under the curve (AUC) and was then compared to clinical parameters followed by multivariate regression analysis. ROC curve analyses revealed a predictive potential for AMACR, HPN, MALAT1, PCA3, and PCAT29 (AUC = 0.614-0.655, p < 0.1). PSA, PSA density, PSA velocity, and MRI maxPI-RADS showed AUC values of 0.681-0.747 (p < 0.05), with accuracies for indicating a PCa risk reclassification of 64-68%. A model including AMACR, MALAT1, PCAT29, PSA density, and MRI maxPI-RADS resulted in an AUC of 0.867 (p < 0.001) with a sensitivity, specificity, and accuracy of 87%, 83%, and 85%, respectively, thus surpassing the predictive power of the individual markers. These findings highlight the potential of uEV transcripts in combination with clinical parameters as monitoring markers during the AS of PCa.
Keywords: active surveillance; biomarker; liquid biopsy; monitoring; prediction; prostate cancer; quantitative PCR; risk reclassification; transcripts; urinary extracellular vesicles.
Conflict of interest statement
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures
Similar articles
-
Urine spermine and multiparametric magnetic resonance imaging for prediction of prostate cancer in Japanese men.Prostate Int. 2023 Sep;11(3):180-185. doi: 10.1016/j.prnil.2023.07.003. Epub 2023 Jul 20. Prostate Int. 2023. PMID: 37745906 Free PMC article.
-
Urine TMPRSS2:ERG Plus PCA3 for Individualized Prostate Cancer Risk Assessment.Eur Urol. 2016 Jul;70(1):45-53. doi: 10.1016/j.eururo.2015.04.039. Epub 2015 May 16. Eur Urol. 2016. PMID: 25985884 Free PMC article.
-
Prognostic accuracy of Prostate Health Index and urinary Prostate Cancer Antigen 3 in predicting pathologic features after radical prostatectomy.Urol Oncol. 2015 Apr;33(4):163.e15-23. doi: 10.1016/j.urolonc.2014.12.002. Epub 2015 Jan 6. Urol Oncol. 2015. PMID: 25575715
-
A novel urinary long non-coding RNA transcript improves diagnostic accuracy in patients undergoing prostate biopsy.Prostate. 2015 May;75(6):653-61. doi: 10.1002/pros.22949. Epub 2015 Jan 18. Prostate. 2015. PMID: 25597901
-
Magnetic resonance imaging on disease reclassification among active surveillance candidates with low-risk prostate cancer: a diagnostic meta-analysis.Prostate Cancer Prostatic Dis. 2015 Sep;18(3):221-8. doi: 10.1038/pcan.2015.20. Epub 2015 May 19. Prostate Cancer Prostatic Dis. 2015. PMID: 25986915 Review.
Cited by
-
Exosomal Liquid Biopsy in Prostate Cancer: A Systematic Review of Biomarkers for Diagnosis, Prognosis, and Treatment Response.Int J Mol Sci. 2025 Jan 18;26(2):802. doi: 10.3390/ijms26020802. Int J Mol Sci. 2025. PMID: 39859516 Free PMC article.
References
-
- Sayyid R.K., Benton J.Z., Reed W.C., Woodruff P., Terris M.K., Wallis C.J.D., Klaassen Z. Prostate cancer mortality rates in low- and favorable intermediate-risk active surveillance patients: A population-based competing risks analysis. World J. Urol. 2023;41:93–99. doi: 10.1007/s00345-022-04228-4. - DOI - PubMed
-
- Cornford P., van den Bergh R.C.N., Briers E., Van den Broeck T., Brunckhorst O., Darraugh J., Eberli D., De Meerleer G., De Santis M., Farolfi A., et al. EAU-EANM-ESTRO-ESUR-ISUP-SIOG Guidelines on Prostate Cancer-2024 Update. Part I: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2024. in press . - DOI - PubMed
-
- Bokhorst L.P., Valdagni R., Rannikko A., Kakehi Y., Pickles T., Bangma C.H., Roobol M.J., for the PRIAS study group A Decade of Active Surveillance in the PRIAS Study: An Update and Evaluation of the Criteria Used to Recommend a Switch to Active Treatment. Eur. Urol. 2016;70:954–960. doi: 10.1016/j.eururo.2016.06.007. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
