

Unsolved Issues in the Integrated Histo-Molecular Classification of Endometrial Carcinoma and Therapeutic Implications
- PMID: 39001520
- PMCID: PMC11240465
- DOI: 10.3390/cancers16132458
Unsolved Issues in the Integrated Histo-Molecular Classification of Endometrial Carcinoma and Therapeutic Implications
Abstract
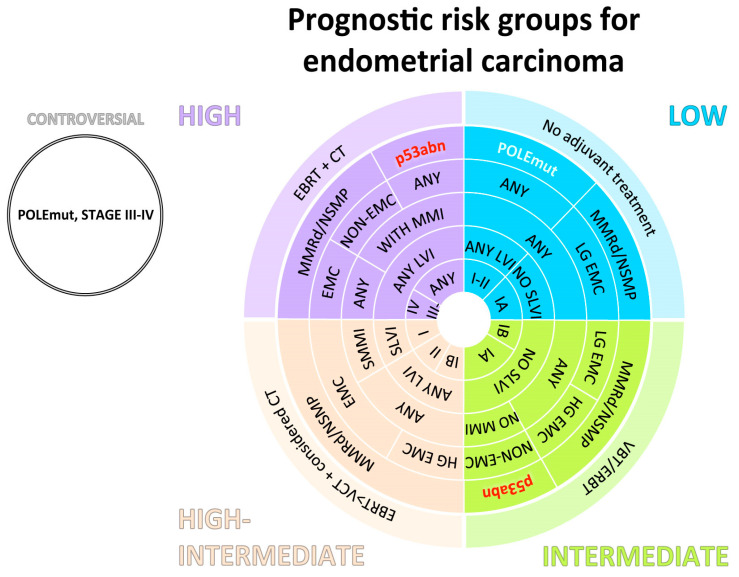
Endometrial carcinoma (EC) is the most frequent gynecological cancer, with an increasing incidence and mortality in recent times. The last decade has represented a true revolution with the development of the integrated histo-molecular classification of EC, which allows for the stratification of patients with morphologically indistinguishable disease into groups with different prognoses. Particularly, the POLE-mutated subgroup exhibits outstanding survival. Nevertheless, the indiscriminate application of molecular classification appears premature. Its prognostic significance has been proven mainly in endometrioid EC, the most common histotype, but it has yet to be convincingly confirmed in the other minor histotypes, which indeed account for a relevant proportion of EC mortality. Moreover, its daily use both requires a mindful pathologist who is able to correctly evaluate and unambiguously report immunohistochemical staining used as a surrogated diagnostic tool and is hampered by the unavailability of POLE mutation analysis. Further molecular characterization of ECs is needed to allow for the identification of better-tailored therapies in different settings, as well as the safe avoidance of surgery for fertility preservation. Hopefully, the numerous ongoing clinical trials in the adjuvant and metastatic settings of EC will likely produce evidence to refine the histo-molecular classification and therapeutic guidelines. Our review aims to retrace the origin and evolution of the molecular classification for EC, reveal its strengths and limitations, show clinical relevance, and uncover the desired future developments.
Keywords: checkpoint inhibitors; classification; endometrial; endometrial cancer; history; targeted therapy.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

Similar articles
-
New therapeutic targets for endometrial cancer: a glimpse into the preclinical sphere.Expert Opin Ther Targets. 2024 Jan-Feb;28(1-2):29-43. doi: 10.1080/14728222.2024.2316739. Epub 2024 Feb 12. Expert Opin Ther Targets. 2024. PMID: 38327111 Review.
-
Endometrial Cancer: Transitioning from Histology to Genomics.Curr Oncol. 2022 Jan 31;29(2):741-757. doi: 10.3390/curroncol29020063. Curr Oncol. 2022. PMID: 35200562 Free PMC article. Review.
-
Biomarker characterization in endometrial cancer in Italy: first survey data analysis.Pathologica. 2022 Jun;114(3):189-198. doi: 10.32074/1591-951X-775. Pathologica. 2022. PMID: 35775705 Free PMC article.
-
Impact of endometrial carcinoma histotype on the prognostic value of the TCGA molecular subgroups.Arch Gynecol Obstet. 2020 Jun;301(6):1355-1363. doi: 10.1007/s00404-020-05542-1. Epub 2020 Apr 15. Arch Gynecol Obstet. 2020. PMID: 32296930
-
TCGA Molecular Prognostic Groups of Endometrial Carcinoma: Current Knowledge and Future Perspectives.Int J Mol Sci. 2022 Oct 2;23(19):11684. doi: 10.3390/ijms231911684. Int J Mol Sci. 2022. PMID: 36232987 Free PMC article. Review.
Cited by
-
The Histomorphology to Molecular Transition: Exploring the Genomic Landscape of Poorly Differentiated Epithelial Endometrial Cancers.Cells. 2025 Mar 5;14(5):382. doi: 10.3390/cells14050382. Cells. 2025. PMID: 40072110 Free PMC article. Review.
References
-
- Scully R.E. Histological Typing of Female Genital Tract Tumours. 2nd ed. Springer; Berlin, Germany: New York, NY, USA: 1994. 189p International histological classification of tumours.
-
- World Health Organization . Female Genital Tumours. 5th ed. World Health Organization; Lyon, France: Geneva, Switzerland: 2020. 632p WHO Classification of Tumours Vol. 4.
