

Unraveling the molecular architecture of autoimmune thyroid diseases at spatial resolution
- PMID: 39003267
- PMCID: PMC11246508
- DOI: 10.1038/s41467-024-50192-5
Unraveling the molecular architecture of autoimmune thyroid diseases at spatial resolution
Abstract
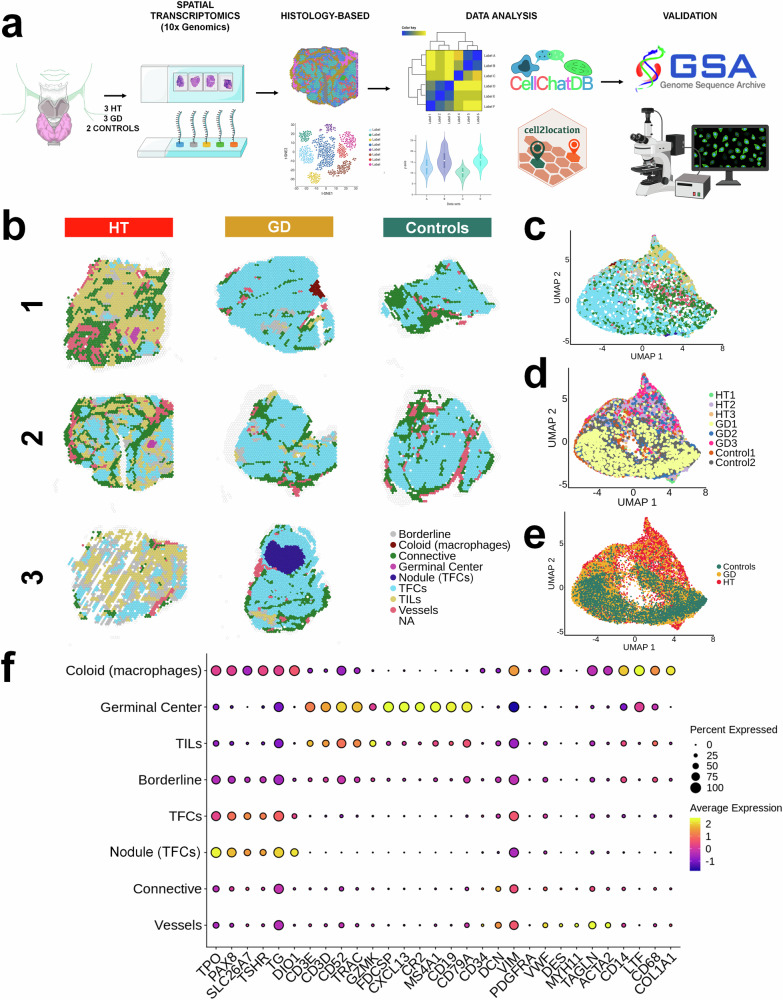
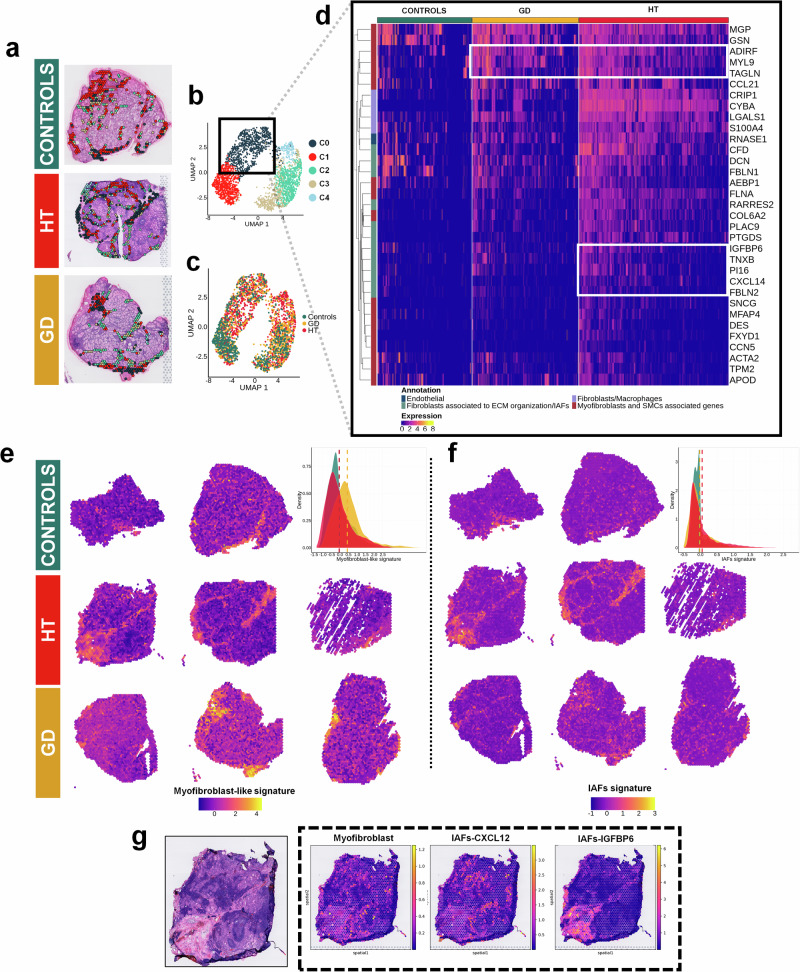
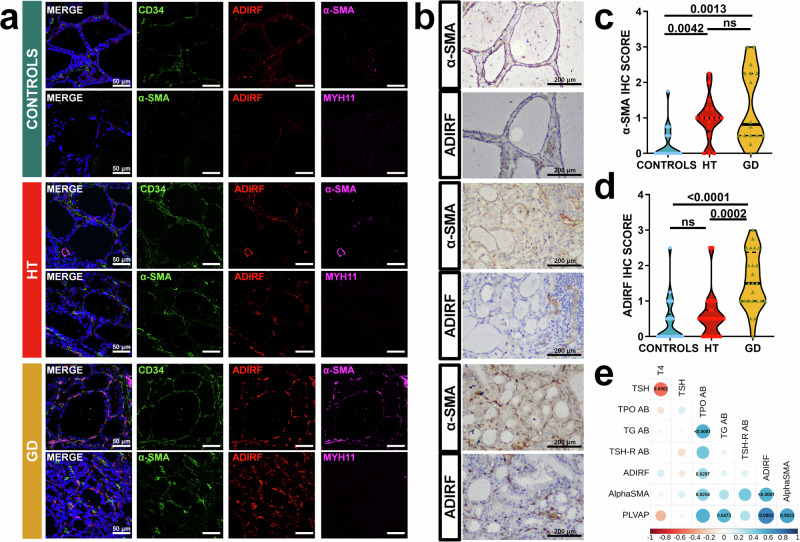
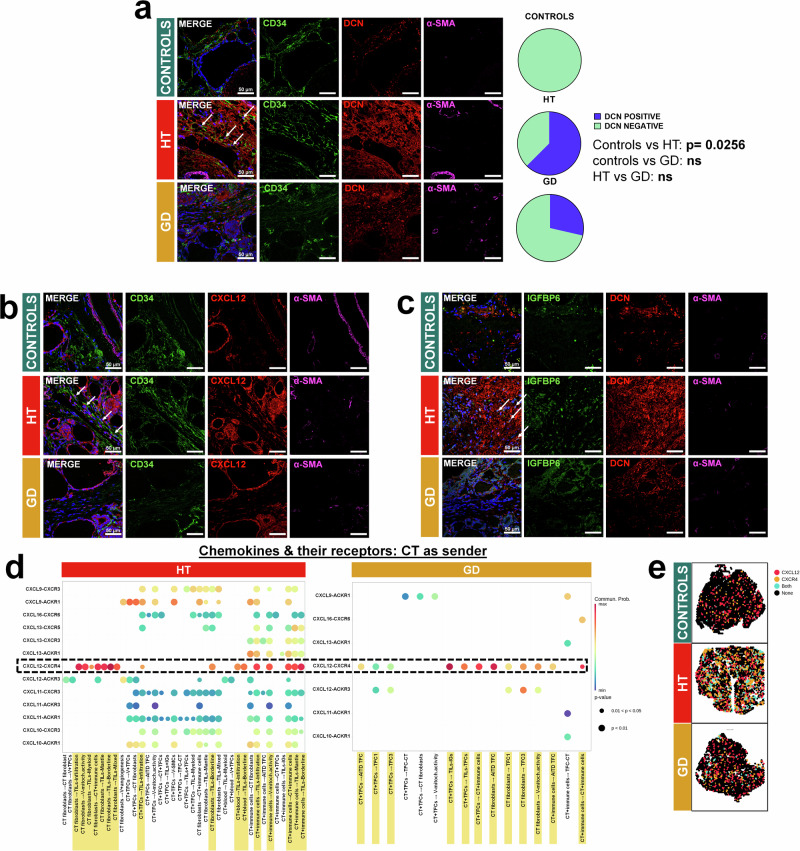
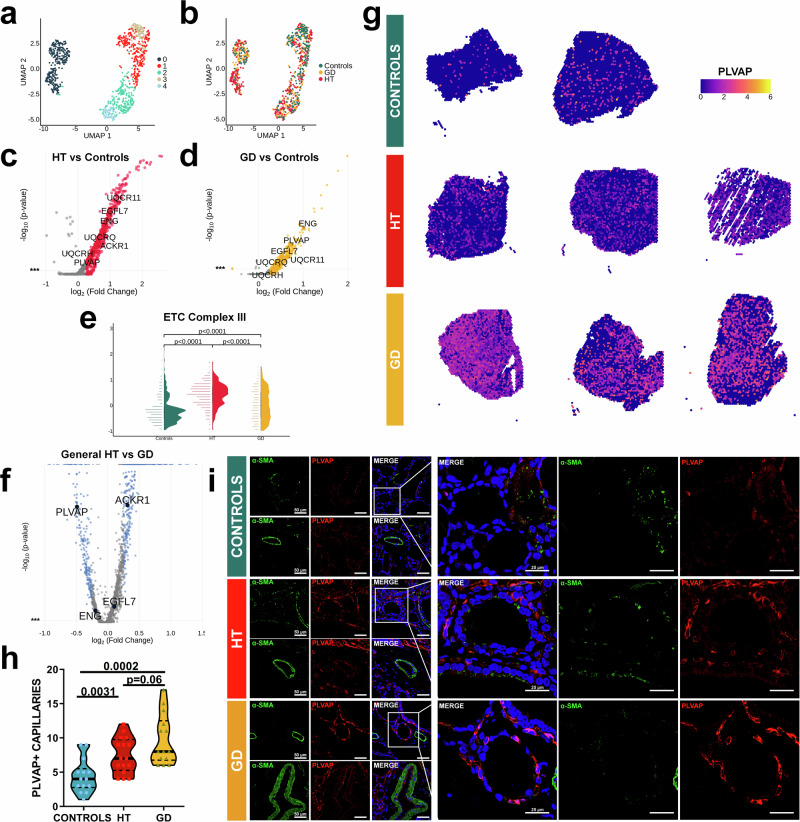
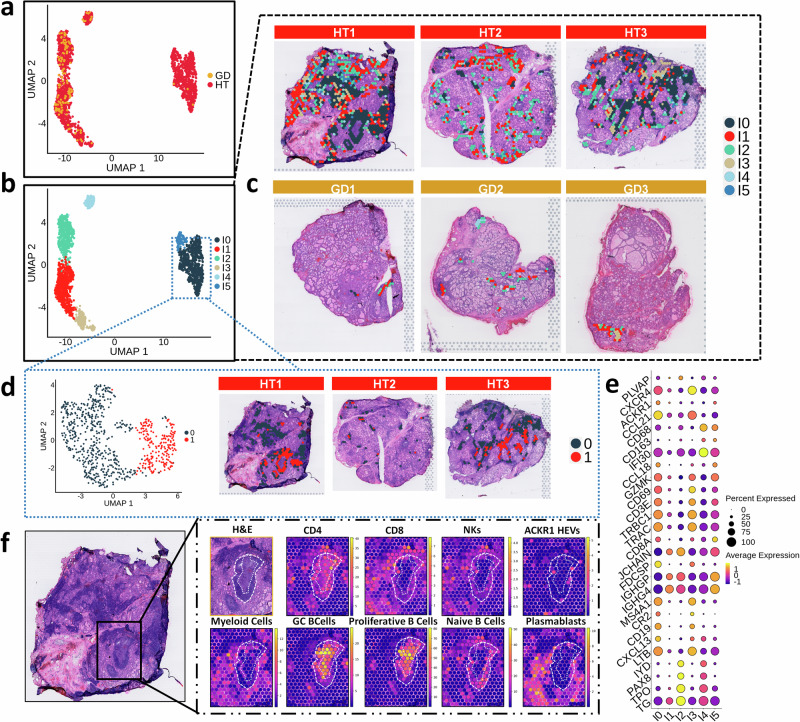
Autoimmune thyroid diseases (AITD) such as Graves' disease (GD) or Hashimoto's thyroiditis (HT) are organ-specific diseases that involve complex interactions between distinct components of thyroid tissue. Here, we use spatial transcriptomics to explore the molecular architecture, heterogeneity and location of different cells present in the thyroid tissue, including thyroid follicular cells (TFCs), stromal cells such as fibroblasts, endothelial cells, and thyroid infiltrating lymphocytes. We identify damaged antigen-presenting TFCs with upregulated CD74 and MIF expression in thyroid samples from AITD patients. Furthermore, we discern two main fibroblast subpopulations in the connective tissue including ADIRF+ myofibroblasts, mainly enriched in GD, and inflammatory fibroblasts, enriched in HT patients. We also demonstrate an increase of fenestrated PLVAP+ vessels in AITD, especially in GD. Our data unveil stromal and thyroid epithelial cell subpopulations that could play a role in the pathogenesis of AITD.
© 2024. The Author(s).
Conflict of interest statement
H.H. is a co-founder and shareholder of Omniscope, a scientific advisory board member of MiRXES and Nanostring, and a consultant to Moderna and Singularity. The remaining authors declare no competing financial or non-financial interests.
Figures


References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
