

Susceptibility gene mutations in germline and tumors of patients with HER2-negative advanced breast cancer
- PMID: 39003306
- PMCID: PMC11246424
- DOI: 10.1038/s41523-024-00667-x
Susceptibility gene mutations in germline and tumors of patients with HER2-negative advanced breast cancer
Abstract
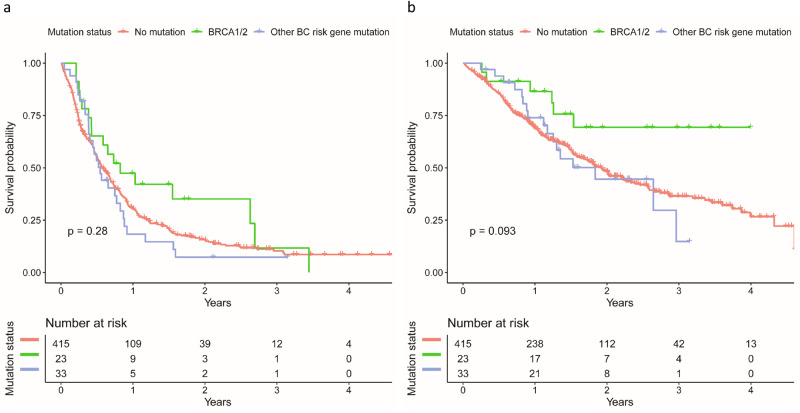
Germline mutations in BRCA1 and BRCA2 (gBRCA1/2) are required for a PARP inhibitor therapy in patients with HER2-negative (HER2-) advanced breast cancer (aBC). However, little is known about the prognostic impact of gBRCA1/2 mutations in aBC patients treated with chemotherapy. This study aimed to investigate the frequencies and prognosis of germline and somatic BRCA1/2 mutations in HER2- aBC patients receiving the first chemotherapy in the advanced setting. Patients receiving their first chemotherapy for HER2- aBC were retrospectively selected from the prospective PRAEGNANT registry (NCT02338167). Genotyping of 26 cancer predisposition genes was performed with germline DNA of 471 patients and somatic tumor DNA of 94 patients. Mutation frequencies, progression-free and overall survival (PFS, OS) according to germline mutation status were assessed. gBRCA1/2 mutations were present in 23 patients (4.9%), and 33 patients (7.0%) had mutations in other cancer risk genes. Patients with a gBRCA1/2 mutation had a better OS compared to non-mutation carriers (HR: 0.38; 95%CI: 0.17-0.86). PFS comparison was not statistically significant. Mutations in other risk genes did not affect prognosis. Two somatic BRCA2 mutations were found in 94 patients without gBRCA1/2 mutations. Most frequently somatic mutated genes were TP53 (44.7%), CDH1 (10.6%) and PTEN (6.4%). In conclusion, aBC patients with gBRCA1/2 mutations had a more favorable prognosis under chemotherapy compared to non-mutation carriers. The mutation frequency of ~5% with gBRCA1/2 mutations together with improved outcome indicates that germline genotyping of all metastatic patients for whom a PARP inhibitor therapy is indicated should be considered.
© 2024. The Author(s).
Conflict of interest statement
A.D.H. received speaker and consultancy honoraria from AstraZeneca, Amgen, Clovis, Daiichi Sankyo, Eisai, GenomicHealth, Gilead, GSK, Hexal, Lilly, MSD, Novartis, Pfizer, Roche, Pierre-Fabre and Seagen and travel support from AstraZeneca, Pfizer, Roche and Gilead. Ar.Ha. received honoraria from AstraZeneca, Cepheid, Merck Sharp & Dohme, Qiagen, Bristol-Myers Squibb, Illumina, Roche, Janssen, Lilly, Agilent, Diaceutics, Ipsen. F.A.T. received honoraria from AstraZeneca and GlaxoSmithKline. T.N.F. received honoraria from Roche, Novartis, Pfizer, AstraZeneca, Merck Sharp & Dohme, Teva, Daiichi Sankyo. E.C.P. received grants from Grail. H.-C.K. received honoraria and travel support from Carl Zeiss meditec, Theraclion, Novartis, Amgen, AstraZeneca, Pfizer, Roche, Daiichi Sankyo, Tesaro, MSD, onkowissen, Eli Lilly, SurgVision, Exact Sciences and Genomic Health and owns stock of Theraclion and Phaon scientific. P.H. received honoraria, unrestricted educational grants and research funding from Amgen, UCB, Novartis, and Pfizer. P.A.F. received honoraria from Novartis, Pfizer, Daiichi Sankyo, AstraZeneca, Eisai, clin-sol, onkowissen, Merck Sharp & Dohme, Lilly, PierreFabre, Seagen, Roche, Hexal and Agendia. His institution conducts research for Biontech and Cepheid. F.J.C. received honoraria from AstraZeneca, QIAGEN and Ambry Genetics. H.T. received honoraria from Novartis, Pfizer, Roche, Lilly, Seagen, and AstraZeneca. J.E. received honoraria from AstraZeneca Roche, Celgene, Novartis, Pfizer, Pierre Fabre, TEVA and travel support from AstraZeneca, Celgene, Pfizer, TEVA and Pierre Fabre. M.P.L. received honoraria from Pfizer, Roche, MSD, Novartis, AstraZeneca, Eisai, medac, Pierre Fabre, Grünenthal, PharmaMar, Exact Sciences and Lilly for advisory boards, lectures and travel support. M.W. received honoraria from AstraZeneca, Celgene and Novartis. D.L. received honoraria from Amgen, AstraZeneca, Celgene, Daiichi Sankyo, Eisai, Loreal, Pfizer, Pierre Fabre, Novartis, Roche and Teva. V.M. reports speaker honoraria from Amgen, Astra Zeneca, Daiichi Sankyo, Eisai, Pfizer, MSD, Novartis, Roche, Teva, Seagen, GSK, consultancy honoraria from Genomic Health, Gilead, Hexal, Roche, Pierre Fabre, Amgen, ClinSol, Novartis, MSD, Daiichi Sankyo, Eisai, Lilly, GSK, other from Novartis, Roche, Seagen, Genentech, outside the submitted work. E.B. received honoraria from Novartis, Pfizer, AstraZeneca, MSD, Lilly, Daiichi Sankyo, Roche and Hexal for consulting and clinical research management activities. D.W. received honoraria from Consal and research funding from Roche, Pfizer, Novartis, AstraZeneca, Boehringer Ingelheim, Daiichi Sankyo. A.S. reports grants from Celgene, grants from Roche, grants from AbbVie, personal fees from Roche, AstraZeneca, Celgene, Pfizer, Novartis, Merck Sharp & Dohme, Tesaro, Lilly, Seagen. S.Y.B. received honoraria from Roche Novartis, Pfizer, AstraZenca and Teva. M.U. received honoraria from Abbvie, Amgen, AstraZeneca, Bristol Myer Squibb, Celgene, Daiichi Sankyo, Eisai, Janssen Cilag, Johnson&Johnson, Lilly, Merck Sharp & Dohme, Mundipharma, Myriad Genetics, Odonate, Pfizer, Puma, Riemser, Roche, Sanofi Aventis, Sividon, and Teva. P.W. received honoraria from AstraZeneca, Merck Sharp & Dohme, Teva, Eisai, Novartis, Pfizer, Roche, Amgen, Pfizer, Tesaro, Pharmamar All remaining authors (L.H., R.D.G., M.R., W.J., S.U., H.H., Al.He., L.A.W., C.G., S.H., A.B.E, M.W.B., C.H., D.A.) have declared no conflicts of interest.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
