

Midregional Proatrial Natriuretic Peptide (MRproANP) is associated with vertebral fractures and low bone density in patients with chronic obstructive pulmonary disease (COPD)
- PMID: 39003487
- PMCID: PMC11245771
- DOI: 10.1186/s12931-024-02902-2
Midregional Proatrial Natriuretic Peptide (MRproANP) is associated with vertebral fractures and low bone density in patients with chronic obstructive pulmonary disease (COPD)
Abstract
Background: Patients with COPD are often affected by loss of bone mineral density (BMD) and osteoporotic fractures. Natriuretic peptides (NP) are known as cardiac markers, but have also been linked to fragility-associated fractures in the elderly. As their functions include regulation of fluid and mineral balance, they also might affect bone metabolism, particularly in systemic disorders such as COPD.
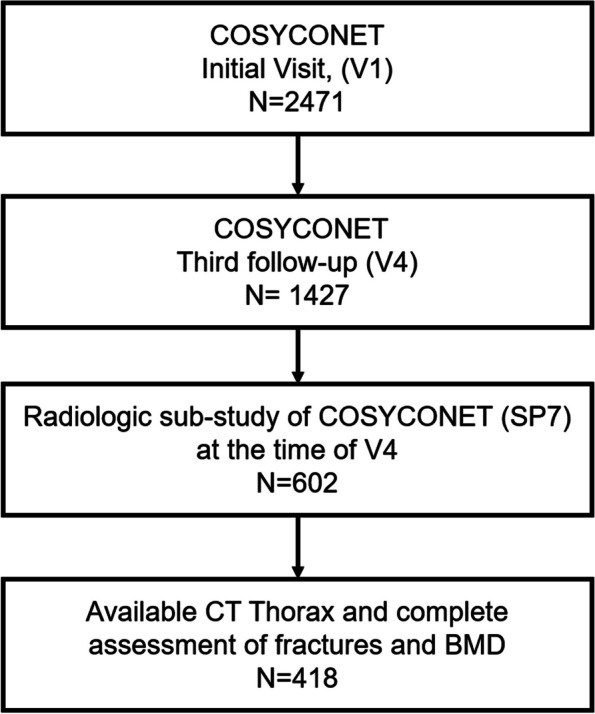
Research question: We investigated the association between NP serum levels, vertebral fractures and BMD assessed by chest computed tomography (CT) in patients with COPD.
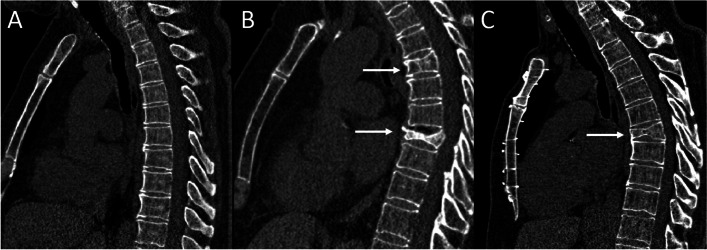
Methods: Participants of the COSYCONET cohort with CT scans were included. Mean vertebral bone density on CT (BMD-CT) as a risk factor for osteoporosis was assessed at the level of TH12 (AI-Rad Companion), and vertebral compression fractures were visually quantified by two readers. Their relationship with N-terminal pro-B-type natriuretic peptide (NT-proBNP), Mid-regional pro-atrial natriuretic peptide (MRproANP) and Midregional pro-adrenomedullin (MRproADM) was determined using group comparisons and multivariable analyses.
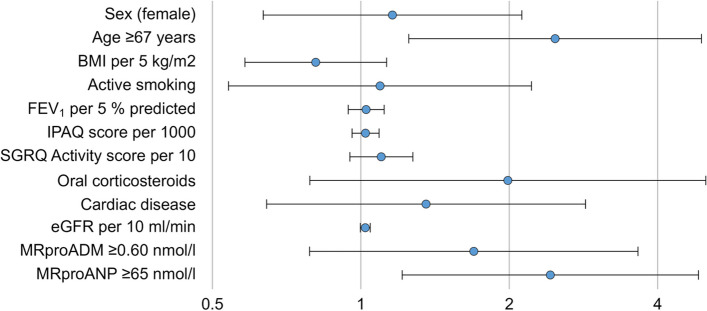
Results: Among 418 participants (58% male, median age 64 years, FEV1 59.6% predicted), vertebral fractures in TH12 were found in 76 patients (18.1%). Compared to patients without fractures, these had elevated serum levels (p ≤ 0.005) of MRproANP and MRproADM. Using optimal cut-off values in multiple logistic regression analyses, MRproANP levels ≥ 65 nmol/l (OR 2.34; p = 0.011) and age (p = 0.009) were the only significant predictors of fractures after adjustment for sex, BMI, smoking status, FEV1% predicted, SGRQ Activity score, daily physical activity, oral corticosteroids, the diagnosis of cardiac disease, and renal impairment. Correspondingly, MRproANP (p < 0.001), age (p = 0.055), SGRQ Activity score (p = 0.061) and active smoking (p = 0.025) were associated with TH12 vertebral density.
Interpretation: MRproANP was a marker for osteoporotic vertebral fractures in our COPD patients from the COSYCONET cohort. Its association with reduced vertebral BMD on CT and its known modulating effects on fluid and ion balance are suggestive of direct effects on bone mineralization.
Trial registration: ClinicalTrials.gov NCT01245933, Date of registration: 18 November 2010.
© 2024. The Author(s).
Conflict of interest statement
FCT reported payments or honoraria for lectures and presentations from Boehringer Ingelheim Chiesi, GlaxoSmithKline, GrifolsNovartis, CSL Behring, Streamed up, RG Gesellschaft für Information and Organisation mbH, PA reports grants from German Federal Ministry of Education and Research (BMBF) Competence Network Asthma and COPD (ASCONET), grants from AstraZeneca GmbH, grants and non-financial support from Bayer Schering Pharma AG, grants, personal fees and non-financial support from Boehringer Ingelheim Pharma GmbH & Co. KG, grants and non-financial support from Chiesi GmbH, grants from GlaxoSmithKline, grants from Grifols Deutschland GmbH, grants from MSD Sharp & Dohme GmbH, grants and personal fees from Mundipharma GmbH, grants, personal fees and non-financial support from Novartis Deutschland GmbH, grants from Pfizer Pharma GmbH, grants from Takeda Pharma Vertrieb GmbH & Co. KG, outside the submitted work. CFV reports grants and personal fees from AstraZeneca, grants and personal fees from Boehringer Ingelheim, grants and personal fees from Chiesi, grants and personal fees from GlaxoSmithKline, grants and personal fees from Grifols, grants and personal fees from Novartis, personal fees from Berlin Chemie/Menarini, personal fees from CSL Behring, grants from German Federal Ministry of Education and Research (BMBF) Competence Network Asthma and COPD (ASCONET), personal fees from Nuvaira, personal fees from MedUpdate, outside the submitted work. HUK reports grants from Siemens, non-financial support from Bayer, during the conduct of the study; grants from Siemens, grants and personal fees from Philips, personal fees from Boehringer Ingelheim, personal fees from Merck Sharp Dohme, personal fees from Astra Zeneca, outside the submitted work. R.B. reports grants and personal fees from AstraZeneca, grants and personal fees from Boehringer Ingelheim, personal fees from GlaxoSmithKline, personal fees from Grifols, grants and personal fees from Novartis, personal fees from CSL Behring, grants from German Federal Ministry of Education and Research (BMBF) Competence Network Asthma and COPD (ASCONET), grants from Sander Stiftung, grants from Schwiete Stiftung, grants from Krebshilfe, grants from Mukoviszidose eV, outside the submitted work. He is Editor in Chief of Respiratory Research. FJF received personal money for adboard activities and lecture fees from Pulmonx, BTG, Olympus and Uptake. RJ, HW, ST, MD, TW, JB, KK, RB, CH, CPC, JB, OvS, SF, EFMW, BW, KFR, VP.
Figures
Similar articles
-
Midregional proatrial naturetic peptide (MRproANP) and copeptin (COPAVP) as predictors of all-cause mortality in recently diagnosed mild to moderate COPD-results from COSYCONET.Respir Res. 2024 Jan 24;25(1):56. doi: 10.1186/s12931-024-02690-9. Respir Res. 2024. PMID: 38267944 Free PMC article.
-
Independent association of bone mineral density and trabecular bone score to vertebral fracture in male subjects with chronic obstructive pulmonary disease.Osteoporos Int. 2018 Mar;29(3):615-623. doi: 10.1007/s00198-017-4314-7. Epub 2017 Nov 22. Osteoporos Int. 2018. PMID: 29167970
-
Associations of daily walking activity with biomarkers related to cardiac distress in patients with chronic obstructive pulmonary disease.Respiration. 2013;85(3):195-202. doi: 10.1159/000345218. Epub 2012 Dec 19. Respiration. 2013. PMID: 23258247
-
Correlation analysis of the vertebral compression degree and CT HU value in elderly patients with osteoporotic thoracolumbar fractures.J Orthop Surg Res. 2023 Jun 26;18(1):457. doi: 10.1186/s13018-023-03941-z. J Orthop Surg Res. 2023. PMID: 37365576 Free PMC article. Review.
-
The impact of chronic obstructive pulmonary disease on bone strength.J Bone Miner Metab. 2024 Jul;42(4):421-427. doi: 10.1007/s00774-024-01496-5. Epub 2024 Feb 7. J Bone Miner Metab. 2024. PMID: 38326630 Review.
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
