

Hereditary angioedema prevalence and satisfaction with prophylaxis in South Australia
- PMID: 39006039
- PMCID: PMC11239692
- DOI: 10.1016/j.waojou.2024.100918
Hereditary angioedema prevalence and satisfaction with prophylaxis in South Australia
Abstract
Background: Hereditary angioedema (HAE) due to deficiency of C1 Inhibitor (C1INH-HAE) is a rare, unpredictable and potentially fatal genetic disorder. There are relatively few systematic population prevalence studies, with reports from various countries of between 1 in 20,000 and 1 in 150,000. and no Australian data. The therapeutic landscape for HAE has changed dramatically in recent years with a focus on highly effective prophylaxis, with the aim of total suppression of angioedema and achievement of a normal life.
Objectives: Epidemiological survey of HAE in South Australia, with description of patient characteristics, quality of life and treatment, with a focus on prophylaxis.
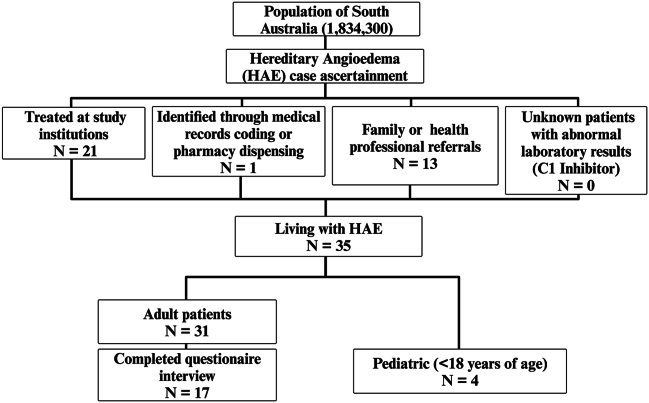
Methods: Case ascertainment was conducted over 18 months from January 2021 to July 2022, using a range of approaches with the aim of identifying all people with C1INH-HAE in South Australia. Questionnaires were administered to consenting patients utilising established HAE-specific and general survey instruments.
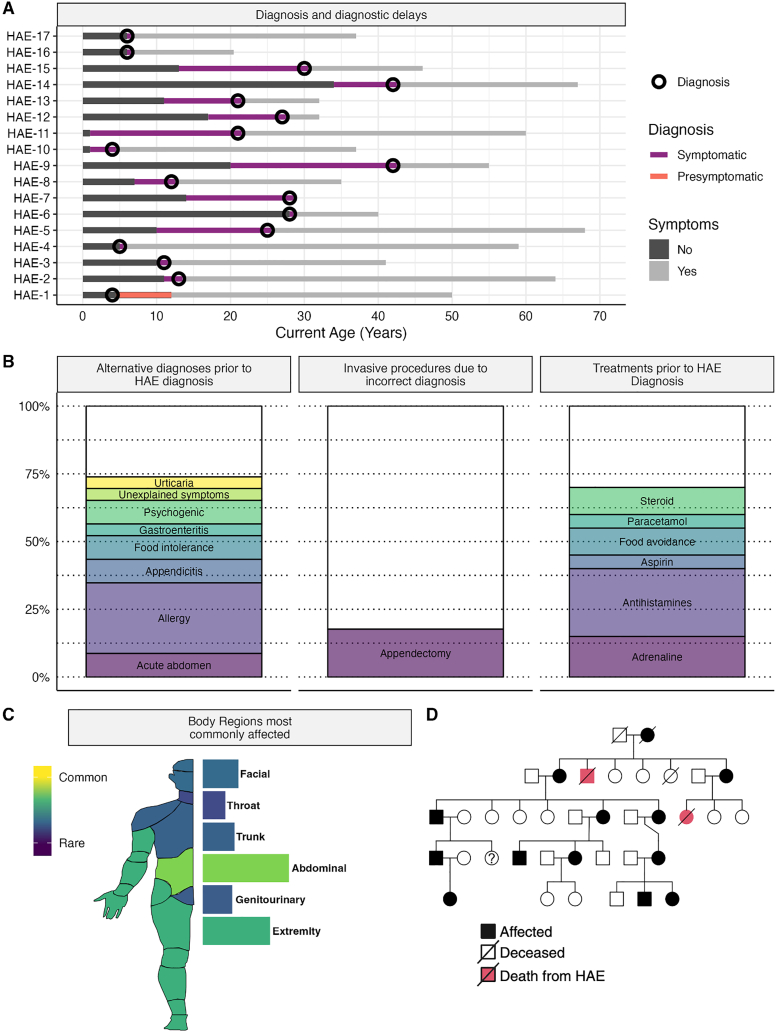
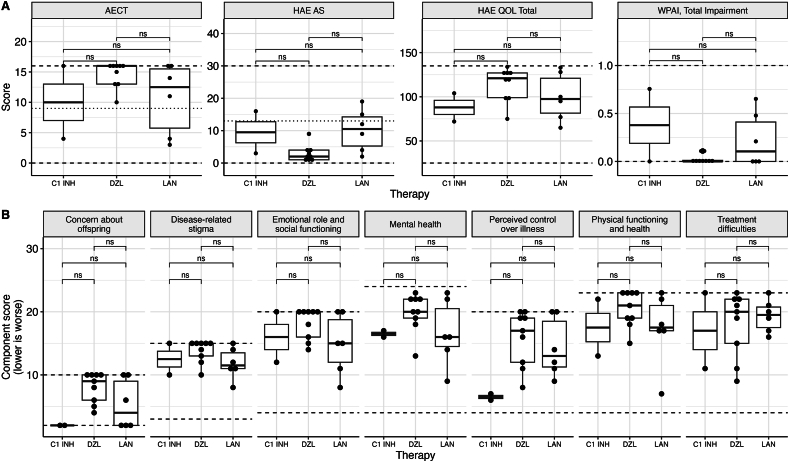
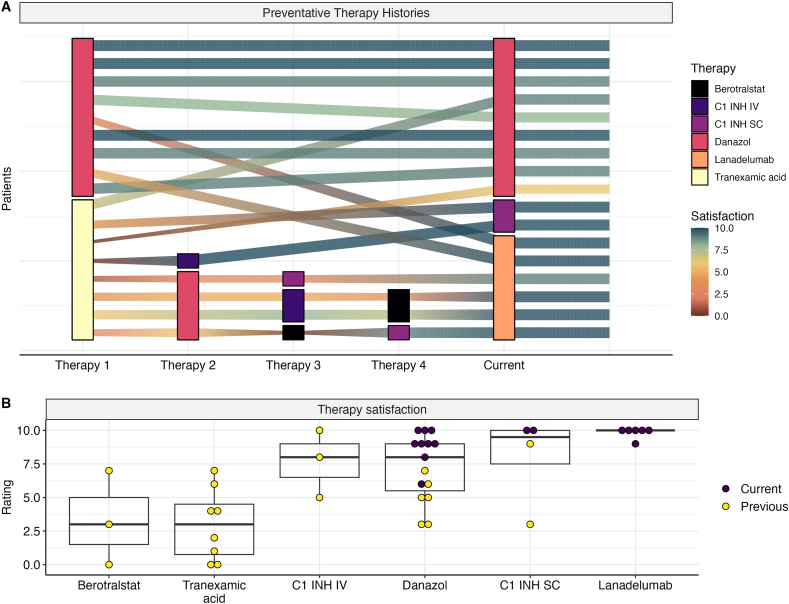
Results: We identified 35 people with HAE in South Australia, yielding a population prevalence of 1 in 52,400, in line with average established international prevalence. HAE was identified in 4 patients of Indigenous Australian heritage. Seventeen of 31 adult patients completed an additional multi-questionnaire survey, revealing overall satisfactory disease control. Most common prophylactic therapies were danazol, lanadelumab, and subcutaneous C1 inhibitor. Many patients (mostly male) with milder disease had responded well to low-dose danazol with good tolerance and have continued to use it, whereas patients with higher disease burden are now using newer therapies, and overall satisfaction with current prophylaxis is high.
Conclusions: Prevalence of HAE in South Australia aligns with international reports. Our population survey indicates that current long-term prophylaxis therapies including danazol, lanadelumab and C1-inhibitor, applied to appropriate patients taking into account disease activity and drug risks and tolerance, are effective for HAE attack prevention and produce high levels of satisfaction.
Keywords: Angioedemas, Hereditary; Angioedemas, Hereditary/therapy; Epidemiology; Health-related quality of life.
Crown Copyright © 2024 Published by Elsevier Inc. on behalf of World Allergy Organization.
Figures
References
-
- Busse P.J., Christiansen S.C. Hereditary angioedema. New England Journal of Medicine [Internet] 2020 Mar 19;382(12):1136–1148. http://www.nejm.org/doi/10.1056/NEJMra1808012 Longo DL, editor. Available from: - DOI - PubMed
-
- Guryanova I., Suffritti C., Parolin D., et al. Hereditary angioedema due to C1 inhibitor deficiency in Belarus: epidemiology, access to diagnosis and seven novel mutations in SERPING1 gene. Clinical and Molecular Allergy [Internet] 2021;19(1):1–8. doi: 10.1186/s12948-021-00141-0. Available from: - DOI - PMC - PubMed
-
- Steiner U.C., Weber-Chrysochoou C., Helbling A., Scherer K., Grendelmeier P.S., Wuillemin W.A. Hereditary angioedema due to C1 – inhibitor deficiency in Switzerland: clinical characteristics and therapeutic modalities within a cohort study. Orphanet J Rare Dis [Internet] 2016;11(1):1–8. doi: 10.1186/s13023-016-0423-1. Available from: - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
