

This is a preprint.
Tumor Regression Following Engineered Polyomavirus-Specific T Cell Therapy in Immune Checkpoint Inhibitor-Refractory Merkel Cell Carcinoma
- PMID: 39006423
- PMCID: PMC11245074
- DOI: 10.1101/2024.07.01.24309780
Tumor Regression Following Engineered Polyomavirus-Specific T Cell Therapy in Immune Checkpoint Inhibitor-Refractory Merkel Cell Carcinoma
Abstract
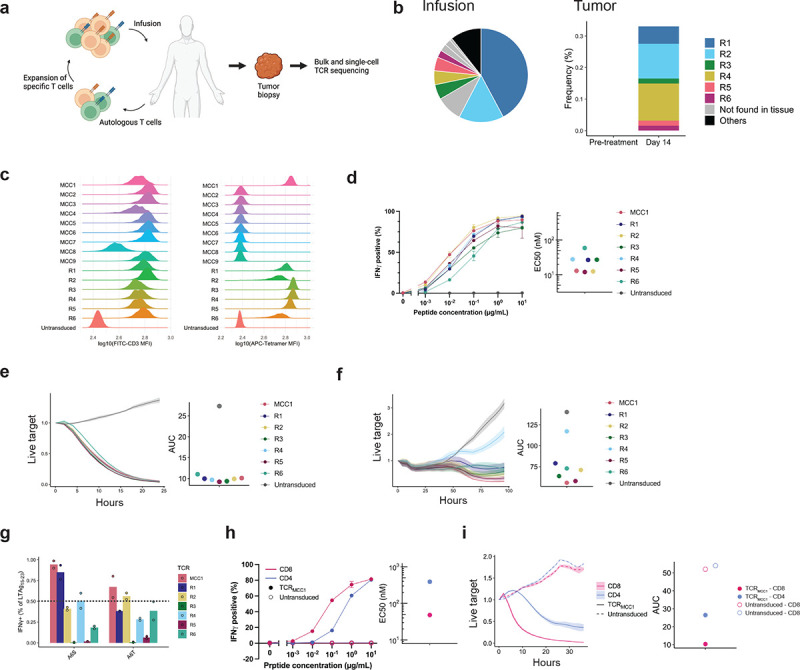
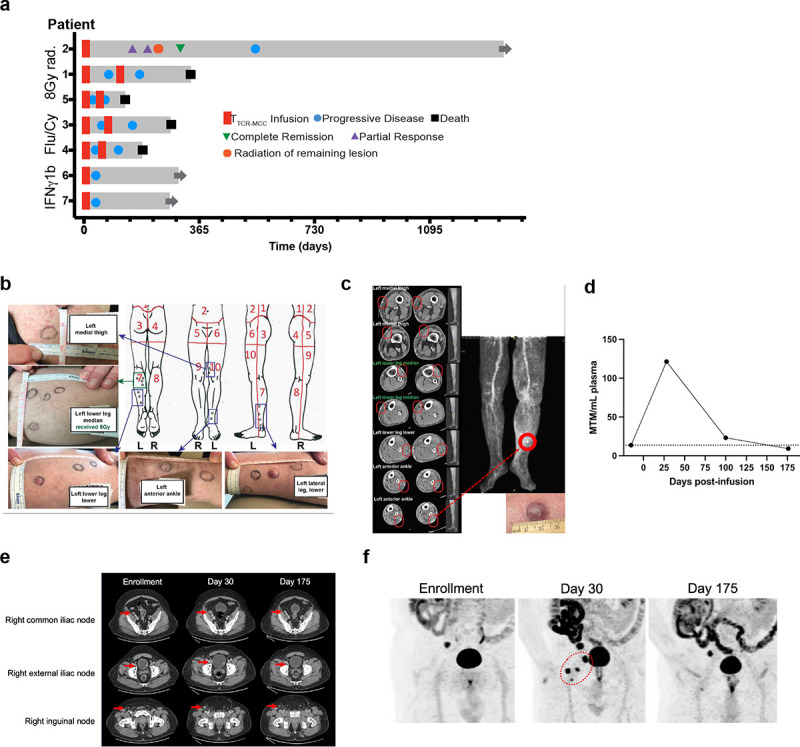
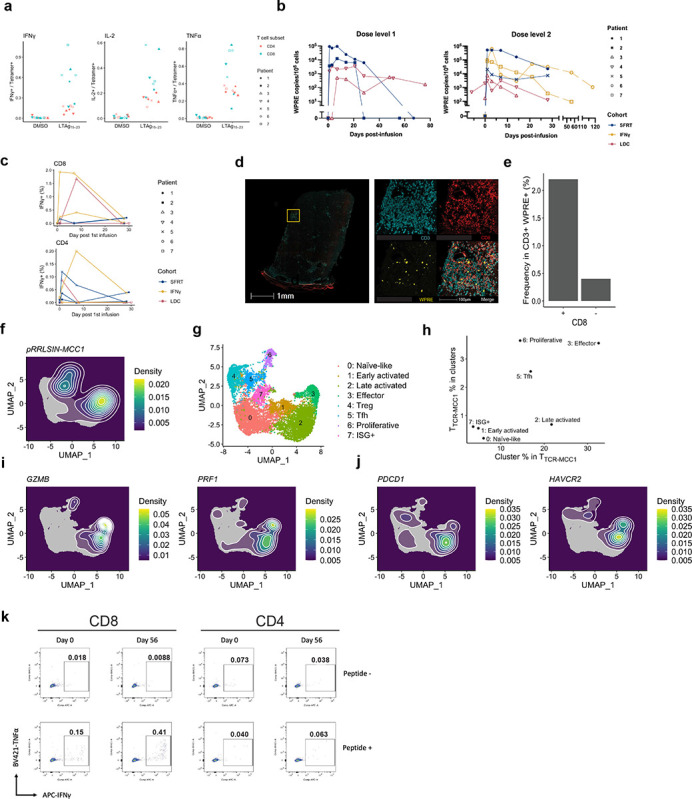
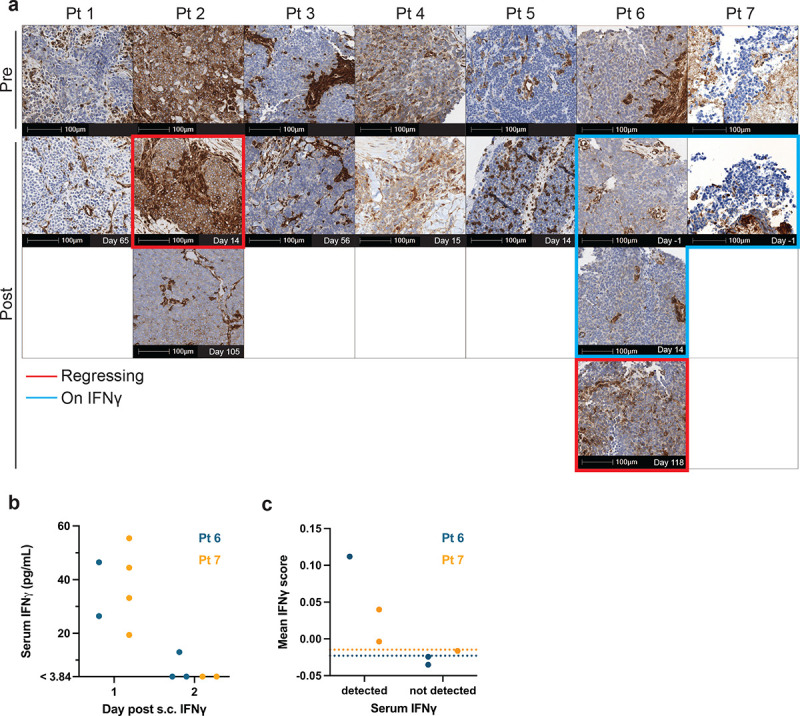
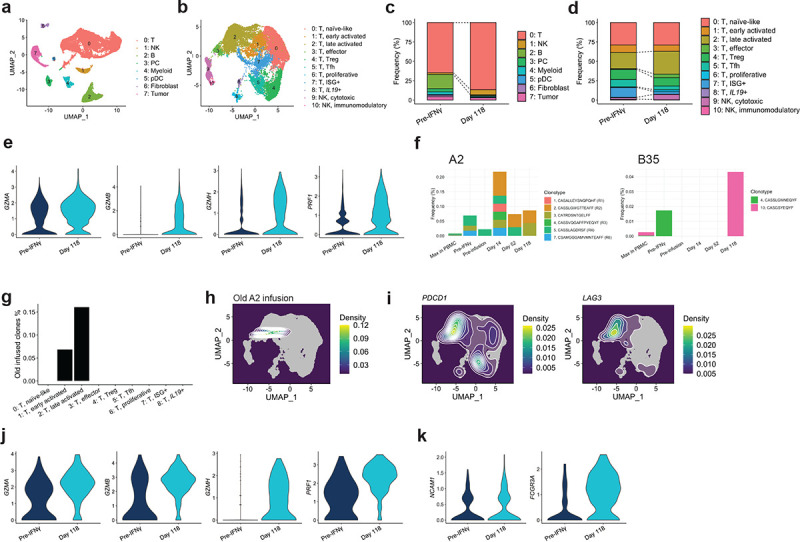
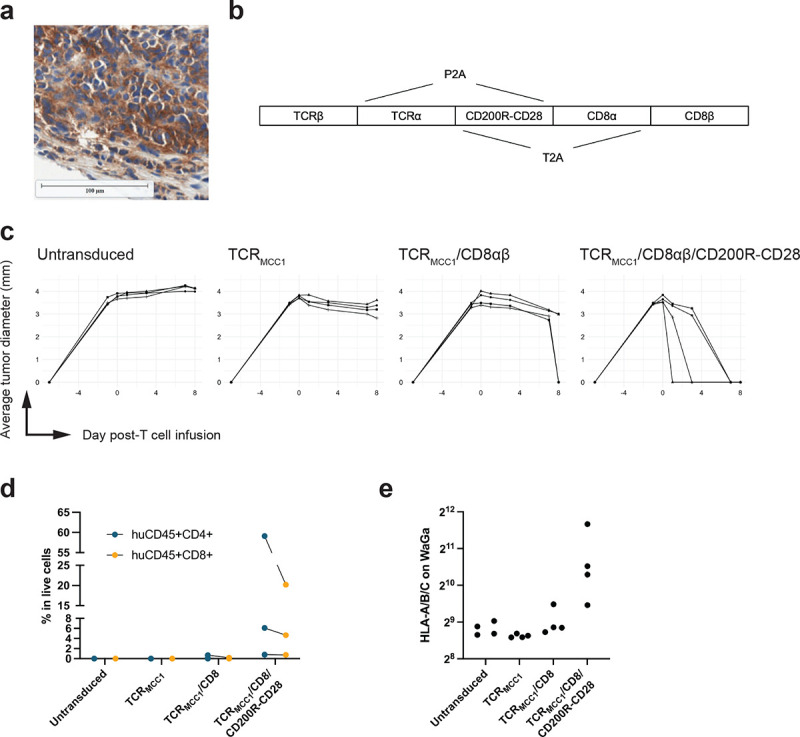
Although immune check-point inhibitors (CPIs) revolutionized treatment of Merkel cell carcinoma (MCC), patients with CPI-refractory MCC lack effective therapy. More than 80% of MCC express T-antigens encoded by Merkel cell polyomavirus, which is an ideal target for T-cell receptor (TCR)-based immunotherapy. However, MCC often repress HLA expression, requiring additional strategies to reverse the downregulation for allowing T cells to recognize their targets. We identified TCRMCC1 that recognizes a T-antigen epitope restricted to human leukocyte antigen (HLA)-A*02:01. Seven CPI-refractory metastatic MCC patients received CD4 and CD8 T cells transduced with TCRMCC1 (TTCR-MCC1) preceded either by lymphodepleting chemotherapy or an HLA-upregulating regimen (single-fraction radiation therapy (SFRT) or systemic interferon gamma (IFNγ)) with concurrent avelumab. Two patients who received preceding SFRT and IFNγ respectively experienced tumor regression. One experienced regression of 13/14 subcutaneous lesions with 1 'escape' lesion and the other had delayed tumor regression in all lesions after initial progression. Although TTCR-MCC1 cells with an activated phenotype infiltrated tumors including the 'escape' lesion, all progressing lesions transcriptionally lacked HLA expression. While SFRT/IFNγ did not immediately upregulate tumor HLA expression, a secondary endogenous antigen-specific T cell infiltrate was detected in one of the regressing tumors and associated with HLA upregulation, indicating in situ immune responses have the potential to reverse HLA downregulation. Indeed, supplying a strong co-stimulatory signal via a CD200R-CD28 switch receptor allows TTCR-MCC1 cells to control HLA-downregulated MCC cells in a xenograft mouse model, upregulating HLA expression. Our results demonstrate the potential of TCR gene therapy for metastatic MCC and propose a next strategy for overcoming epigenetic downregulation of HLA in MCC.
Conflict of interest statement
M. McAfee, P. Nghiem, T. Schmitt and A. G. Chapuis are inventors on Fred Hutchinson patents related to the MCPyV TCR (patent no. 17-085-US-PCT) used in these studies. A. G. Chapuis received research funding through cooperative research and development agreements with bluebird Bio and Affini-T Therapeutics.
Figures
References
-
- Cowey C. L. et al. Real-world treatment outcomes in patients with metastatic Merkel cell carcinoma treated with chemotherapy in the USA. Future Oncology 13, 1699–1710 (2017). - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials