

Understanding the relationship between HCV infection and progression of kidney disease
- PMID: 39006752
- PMCID: PMC11239345
- DOI: 10.3389/fmicb.2024.1418301
Understanding the relationship between HCV infection and progression of kidney disease
Abstract
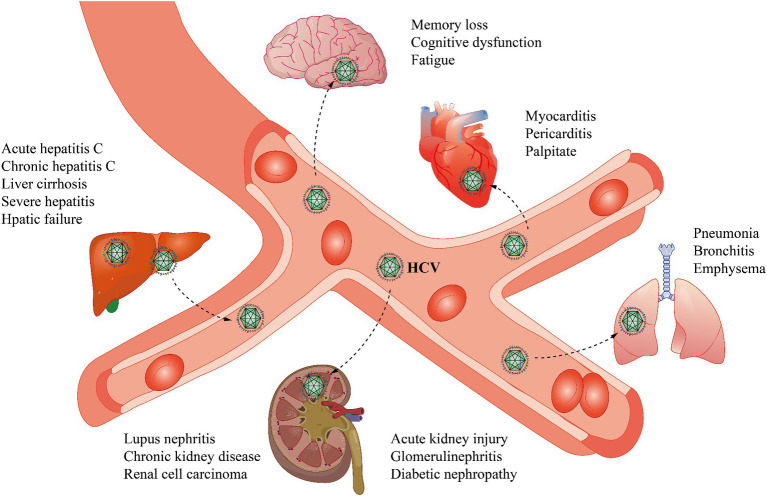
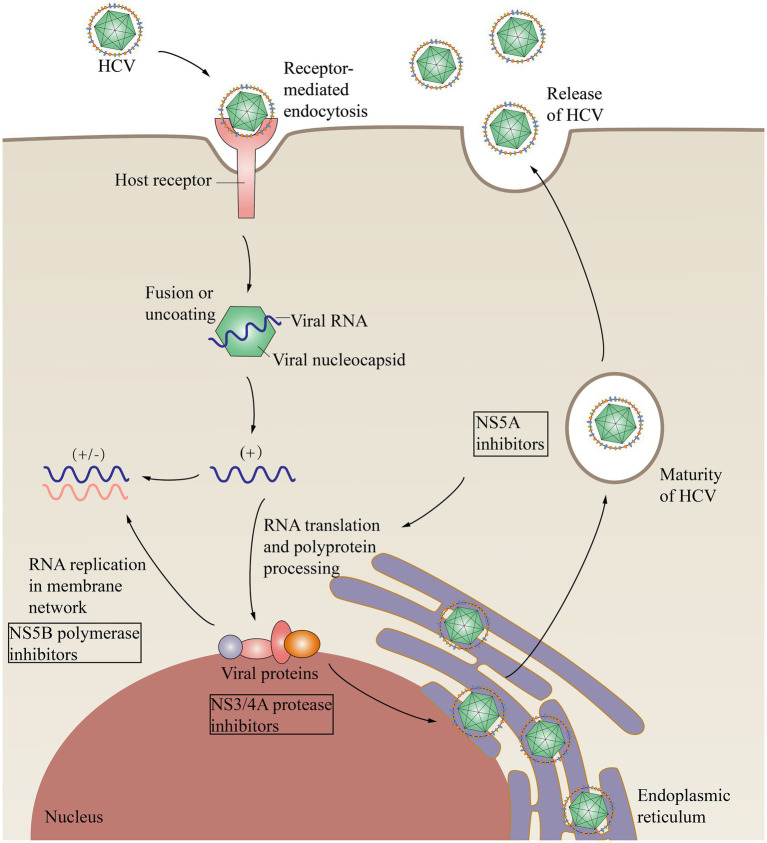
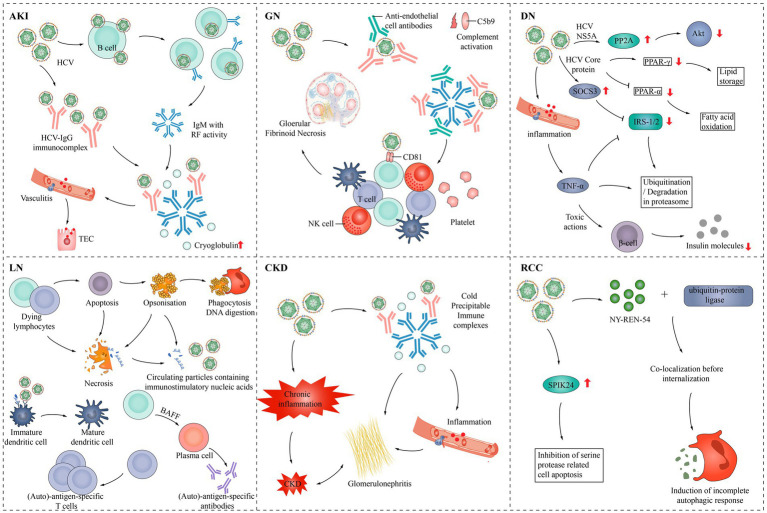
Hepatitis C virus (HCV) can cause a range of kidney diseases. HCV is the primary cause of mixed cryoglobulinaemia, which leads to cryoglobulinaemic vasculitis and cryoglobulinaemic glomerulonephritis (GN). Patients with acute cryoglobulinaemic vasculitis often exhibit acute kidney disease due to HCV infection, which typically progresses to acute kidney injury (AKI). HCV also increases the risk of chronic kidney disease (CKD) and the likelihood of developing end-stage renal disease (ESRD). Currently, direct-acting antiviral agents (DAAs) can be used to treat kidney disease at different stages. This review focuses on key findings regarding HCV and kidney disease, discusses the impact of DAAs, and highlights the need for further research and treatment.
Keywords: acute kidney injury; cryoglobulinaemia; diabetic nephropathy; glomerulonephritis; hepatitis C virus; lupus nephritis; renal cell carcinoma.
Copyright © 2024 Zhang, Han, Lin, Jin, Zhou, Wang, Tang, Li, Li and Chen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources