

Sclerostin inhibition in rare bone diseases: Molecular understanding and therapeutic perspectives
- PMID: 39007037
- PMCID: PMC11245887
- DOI: 10.1016/j.jot.2024.05.004
Sclerostin inhibition in rare bone diseases: Molecular understanding and therapeutic perspectives
Abstract
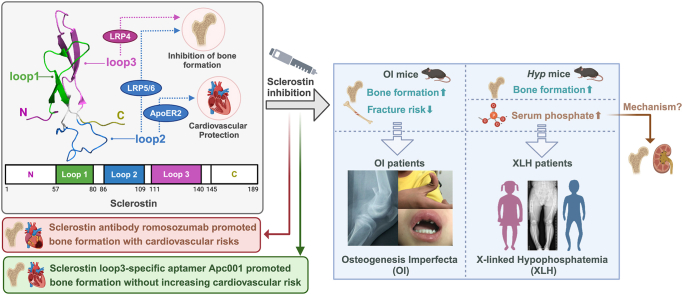
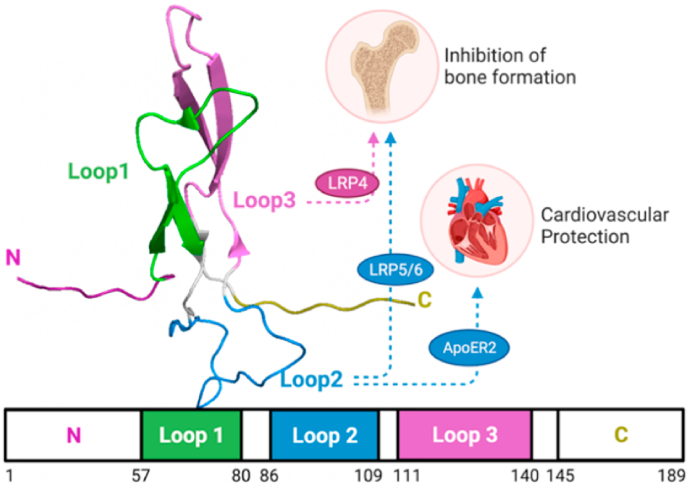
Sclerostin emerges as a novel target for bone anabolic therapy in bone diseases. Osteogenesis imperfecta (OI) and X-linked hypophosphatemia (XLH) are rare bone diseases in which therapeutic potential of sclerostin inhibition cannot be ignored. In OI, genetic/pharmacologic sclerostin inhibition promoted bone formation of mice, but responses varied by genotype and age. Serum sclerostin levels were higher in young OI-I patients, while lower in adult OI-I/III/IV. It's worth investigating whether therapeutic response of OI to sclerostin inhibition could be clinically predicted by genotype and age. In XLH, preclinical/clinical data suggested factors other than identified FGF23 contributing to XLH. Higher levels of circulating sclerostin were detected in XLH. Sclerostin inhibition promoted bone formation in Hyp mice, while restored phosphate homeostasis in age-/gender-dependent manner. The role of sclerostin in regulating phosphate metabolism deserves investigation. Sclerostin/FGF23 levels of XLH patients with/without response to FGF23-antibody warrants study to develop precise sclerostin/FGF23 inhibition strategy or synergistic/additive strategy. Notably, OI patients were associated with cardiovascular abnormalities, so were XLH patients receiving conventional therapy. Targeting sclerostin loop3 promoted bone formation without cardiovascular risks. Further, blockade of sclerostin loop3-LRP4 interaction while preserving sclerostin loop2-ApoER2 interaction could be a potential precise sclerostin inhibition strategy for OI and XLH with cardiovascular safety. The Translational Potential of this Article. Preclinical data on the molecular understanding of sclerostin inhibition in OI and therapeutic efficacy in mouse models of different genotypes, as well as clinical data on serum sclerostin levels in patients with different phenotypes of OI, were reviewed and discussed. Translationally, it would facilitate to develop clinical prediction strategies (e.g. based on genotype and age, not just phenotype) for OI patients responsive to sclerostin inhibition. Both preclinical and clinical data suggested sclerostin as another factor contributing to XLH, in addition to the identified FGF23. The molecular understanding and therapeutic effects of sclerostin inhibition on both promoting bone anabolism and improving phosphate homostasis in Hyp mice were reviewed and discussed. Translationaly, it would facilitate the development of precise sclerostin/FGF23 inhibition strategy or synergistic/additive strategy for the treatment of XLH. Cardiovascular risk could not be ruled out during sclerostin inhibition treatment, especially for OI and XLH patients with cardiovascular diseases history and cardiovascular abnormalities. Studies on the role of sclerostin in inhiting bone formation and protecting cardiovascular system were reviewed and discussed. Translationaly, blockade of sclerostin loop3-LRP4 interaction while preserving sclerostin loop2-ApoER2 interaction could be a potential precise sclerostin inhibition strategy for OI and XLH with cardiovascular safety.
Keywords: Cardiovascular safety; Loops; Osteogenesis imperfecta (OI); Sclerostin; Sclerostin inhibition; Therapeutic perspectives; X-linked hypophosphatemia (XLH).
© 2024 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Therapeutic aptamer targeting sclerostin loop3 for promoting bone formation without increasing cardiovascular risk in osteogenesis imperfecta mice.Theranostics. 2022 Jul 18;12(13):5645-5674. doi: 10.7150/thno.63177. eCollection 2022. Theranostics. 2022. PMID: 35966595 Free PMC article.
-
Sclerostin antibody improves phosphate metabolism hormones, bone formation rates, and bone mass in adult Hyp mice.Bone. 2022 Jan;154:116201. doi: 10.1016/j.bone.2021.116201. Epub 2021 Sep 16. Bone. 2022. PMID: 34537437 Free PMC article.
-
Serum Sclerostin and Its Association with Bone Turnover Marker in Metabolic Bone Diseases.Dis Markers. 2022 Sep 10;2022:7902046. doi: 10.1155/2022/7902046. eCollection 2022. Dis Markers. 2022. PMID: 36124027 Free PMC article.
-
FGF23 and its role in X-linked hypophosphatemia-related morbidity.Orphanet J Rare Dis. 2019 Feb 26;14(1):58. doi: 10.1186/s13023-019-1014-8. Orphanet J Rare Dis. 2019. PMID: 30808384 Free PMC article. Review.
-
What are the benefits of the anti-FGF23 antibody burosumab on the manifestations of X-linked hypophosphatemia in adults in comparison with conventional therapy? A review.Ther Adv Rare Dis. 2022 Feb 21;3:26330040221074702. doi: 10.1177/26330040221074702. eCollection 2022 Jan-Dec. Ther Adv Rare Dis. 2022. PMID: 37180412 Free PMC article. Review.
Cited by
-
Understanding pathophysiology and injury mechanisms is the foundation for invention/innovation and clinical translation in orthopaedics.J Orthop Translat. 2024 Jul 12;47:A1-A2. doi: 10.1016/j.jot.2024.07.003. eCollection 2024 Jul. J Orthop Translat. 2024. PMID: 39161656 Free PMC article. No abstract available.
-
Effect of lipopolysaccharides and mixed Eimeria spp. challenge on performance and bone development in broilers.Poult Sci. 2025 Jun 27;104(10):105501. doi: 10.1016/j.psj.2025.105501. Online ahead of print. Poult Sci. 2025. PMID: 40633317 Free PMC article.
References
-
- Piters E., Culha C., Moester M., Van Bezooijen R., Adriaensen D., Mueller T., et al. First missense mutation in the SOST gene causing sclerosteosis by loss of sclerostin function. Hum Mutat. 2010;31(7):E1526–E1543. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
