

Development of tuberculosis treatment decision algorithms in children below 5 years hospitalised with severe acute malnutrition in Zambia and Uganda: a prospective diagnostic cohort study
- PMID: 39007063
- PMCID: PMC11245985
- DOI: 10.1016/j.eclinm.2024.102688
Development of tuberculosis treatment decision algorithms in children below 5 years hospitalised with severe acute malnutrition in Zambia and Uganda: a prospective diagnostic cohort study
Abstract
Background: In children with severe acute malnutrition (SAM) tuberculosis is common, challenging to diagnose, and often fatal. We developed tuberculosis treatment decision algorithms (TDAs) for children under the age of 5 years with SAM.
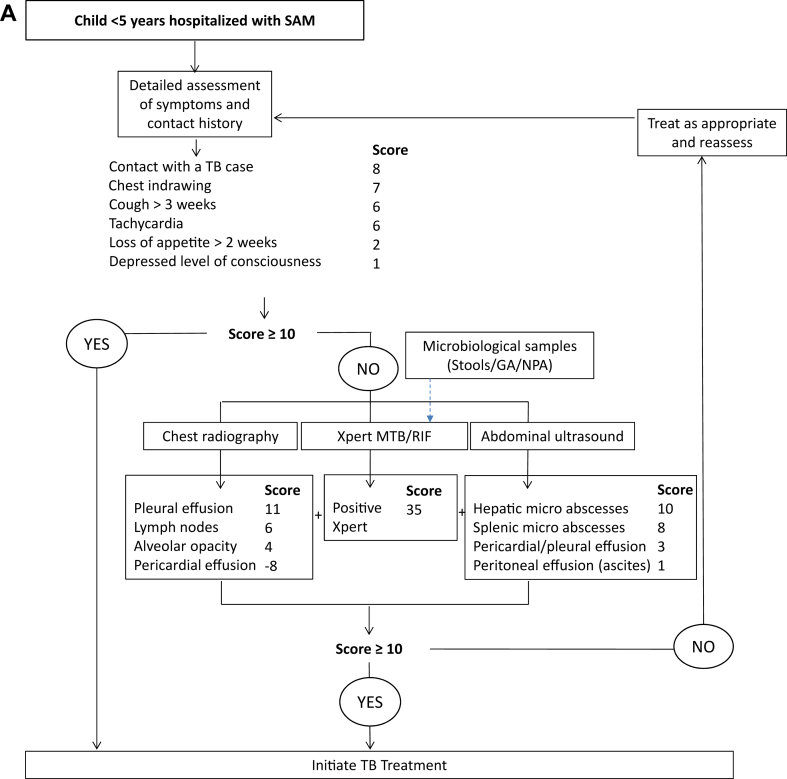
Methods: In this prospective diagnostic study, we enrolled and followed up children aged <60 months hospitalised with SAM at three tertiary hospitals in Zambia and Uganda from 4 November 2019 to 20 June 2022. We included children aged 2-59 months with SAM as defined by WHO and hospitalised following the WHO clinical criteria. We excluded children with current or history of antituberculosis treatment within the preceding 3 months. They underwent tuberculosis symptom screening, clinical assessment, chest X-ray, abdominal ultrasound, Xpert MTB/RIF Ultra (Ultra) and culture on respiratory and stool samples with 6 months follow-up. Tuberculosis was retrospectively defined using the 2015 standard case definition for childhood tuberculosis. We used logistic regression to develop diagnostic prediction models for a one-step diagnosis and a two-step screening and diagnostic approaches. We derived scores from models using WHO-recommended thresholds for sensitivity and proposed TDAs. This study is registered with ClinicalTrials.gov, NCT04240990.
Findings: Of 1906 children hospitalised with SAM during the study period, 1230 were screened, 1152 were eligible and 603 were enrolled. Of the 603 children enrolled-median age 15 (inter-quartile range (IQR): 11-20) months and 65 (11.0%) living with HIV-114 (18.9%) were diagnosed with tuberculosis, including 51 (8.5%) with microbiological confirmation and 104 (17.2%) initiated treatment at a median of 6(IQR: 2-10) days after inclusion. 108 children were retrospectively classified as having tuberculosis resulting in a prevalence of 17.9% (95% confidence intervals (CI): 15.1; 21.2). 75 (69.4%) children with tuberculosis reported cough of any duration, 32 (29.6%) cough ≥2 weeks and 11 (10.2%) tuberculosis contact history. 535 children had complete data and were included in the diagnostic prediction model. The one-step diagnostic model had 15 predictors, including Ultra, clinical, radiographic, and abdominal features, an area under the receiving operating curve (AUROC) of 0.910, and derived TDA sensitivity of 86.14% (95% CI: 78.07-91.56) and specificity of 80.88% (95% CI: 76.91-84.30). The two-step model had AUROCs of 0.750 and 0.912 for screening and diagnosis, respectively, and derived combined TDA sensitivity of 79.21% (95% CI: 70.30-85.98) and a specificity of 83.64% (95% CI: 79.87-86.82).
Interpretation: Tuberculosis prevalence was high among hospitalised children with SAM, with atypical clinical features. TDAs achieved satisfactory diagnostic accuracy and could be used to improve diagnosis in this vulnerable group.
Funding: Unitaid.
Keywords: Children; Diagnosis; Severe acute malnutrition; Treatment decision algorithms; Tuberculosis.
© 2024 The Author(s).
Conflict of interest statement
All authors declare no competing interests.
Figures




References
-
- World-Health-Organisation . World Health Organisation; Geneva: 2023. Global tuberculosis report 2023.
-
- Unicef-WHO-World-Bank-Group . World Health Organisation and World Bank Group; 2023. Levels and trends in child malnutrition-Unicef/WHO/World bank joint child malnutrition estimates New York UNICEF.
-
- Black R.E., Victora C.G., Walker S.P., et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet. 2013;382(9890):427–451. - PubMed
-
- World-Health-Organisation. Guideline . World Health Organisation; Geneva: 2013. Updates on the management of acute severe malnutrition in infants and children. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
