

Anti-inflammatory therapy with nebulized dornase alfa for severe COVID-19 pneumonia: a randomized unblinded trial
- PMID: 39009040
- PMCID: PMC11251720
- DOI: 10.7554/eLife.87030
Anti-inflammatory therapy with nebulized dornase alfa for severe COVID-19 pneumonia: a randomized unblinded trial
Abstract
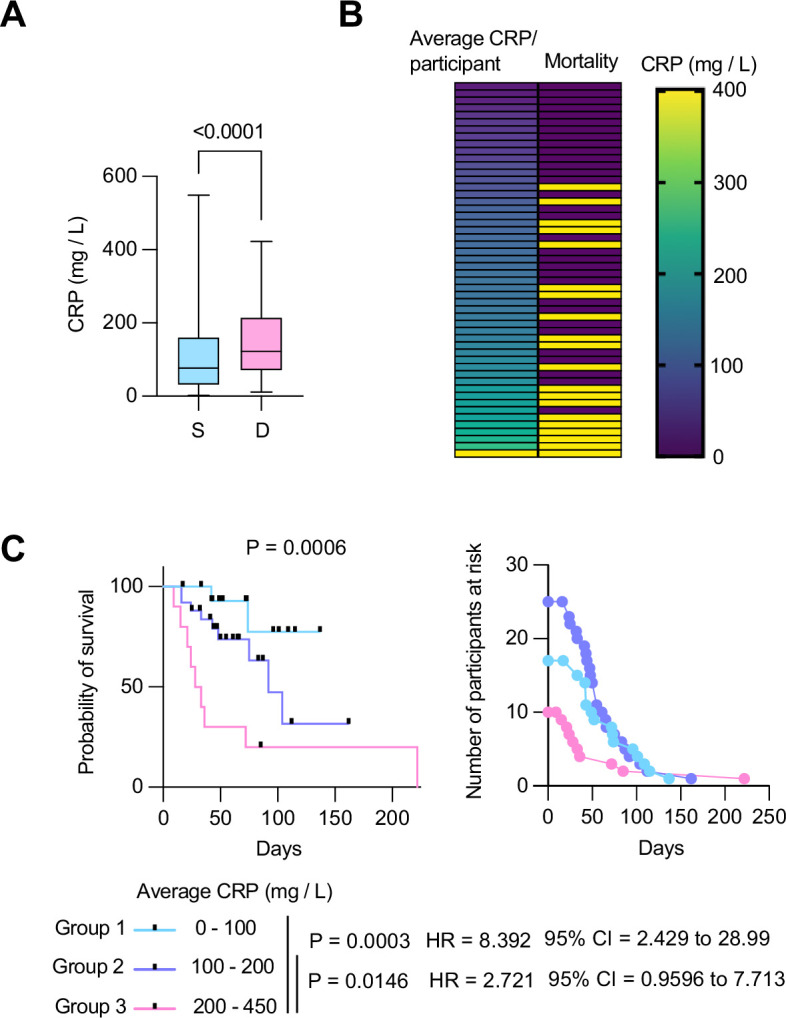
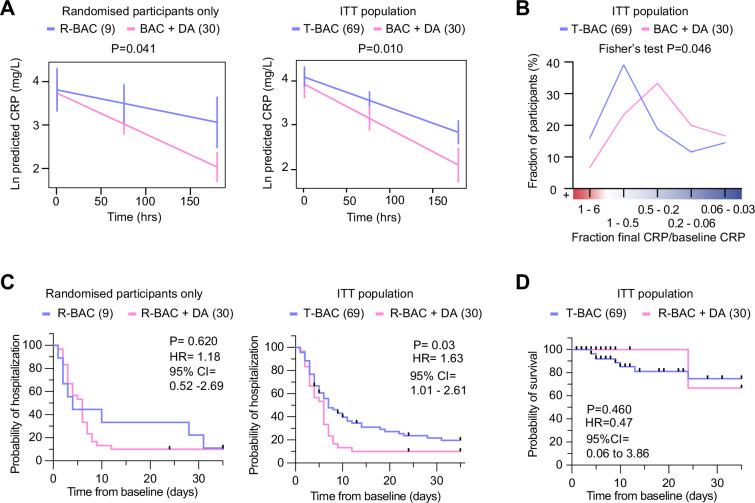
Background: Prinflammatory extracellular chromatin from neutrophil extracellular traps (NETs) and other cellular sources is found in COVID-19 patients and may promote pathology. We determined whether pulmonary administration of the endonuclease dornase alfa reduced systemic inflammation by clearing extracellular chromatin.
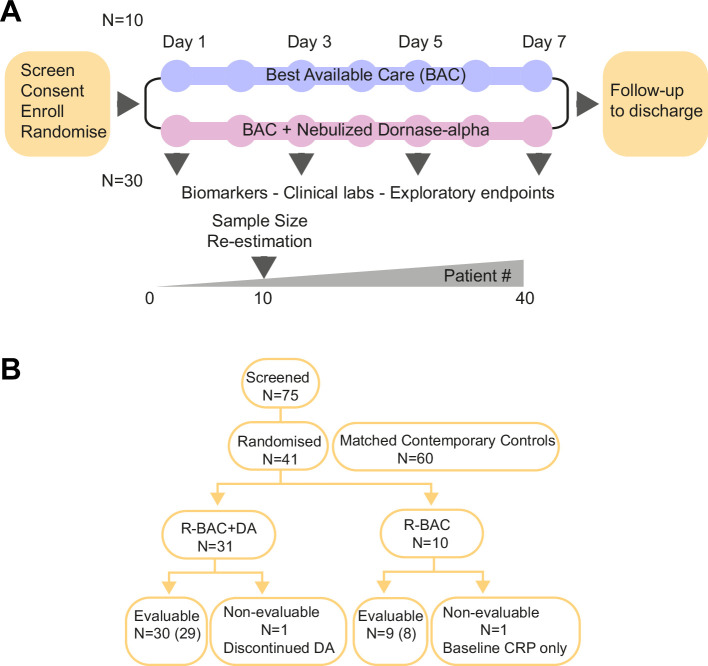
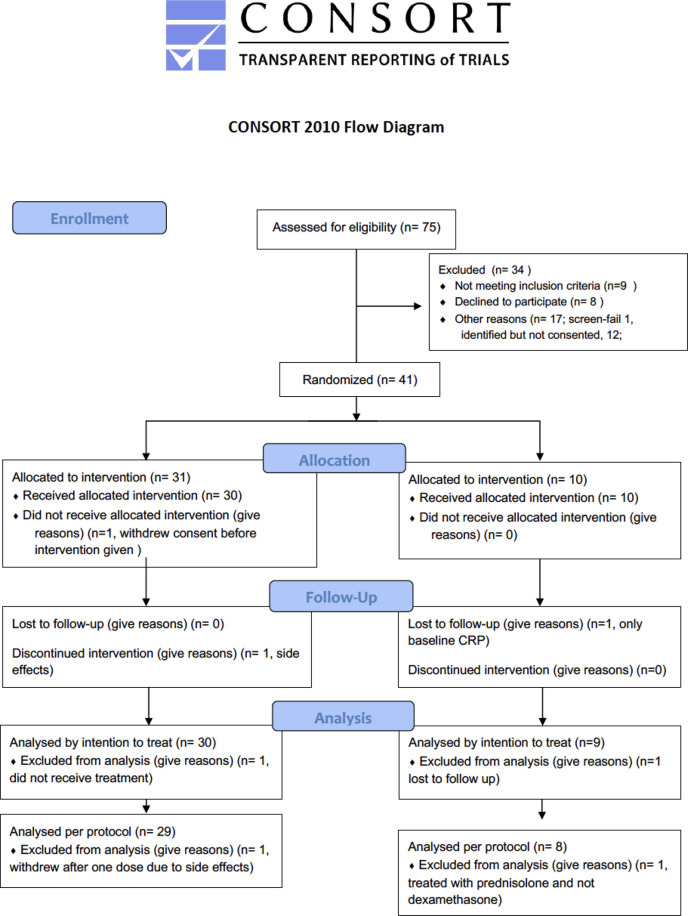
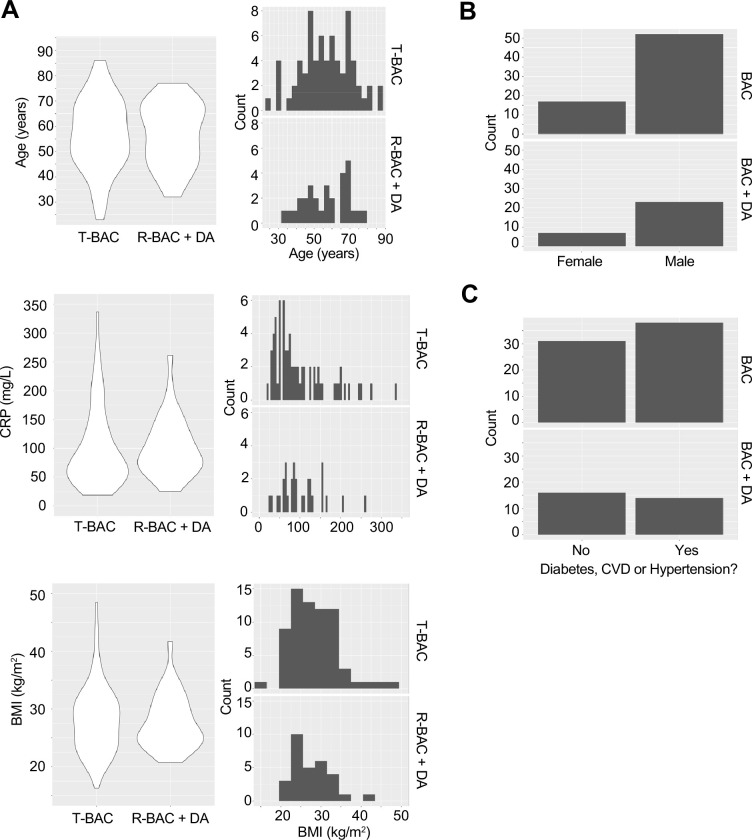
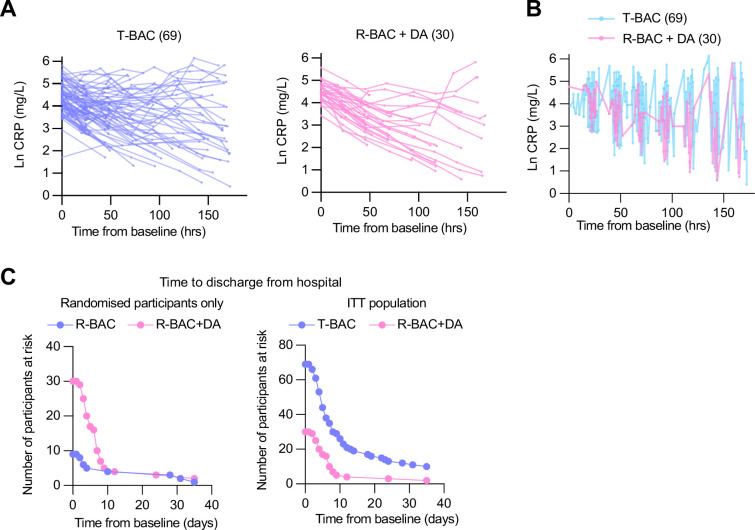
Methods: Eligible patients were randomized (3:1) to the best available care including dexamethasone (R-BAC) or to BAC with twice-daily nebulized dornase alfa (R-BAC + DA) for seven days or until discharge. A 2:1 ratio of matched contemporary controls (CC-BAC) provided additional comparators. The primary endpoint was the improvement in C-reactive protein (CRP) over time, analyzed using a repeated-measures mixed model, adjusted for baseline factors.
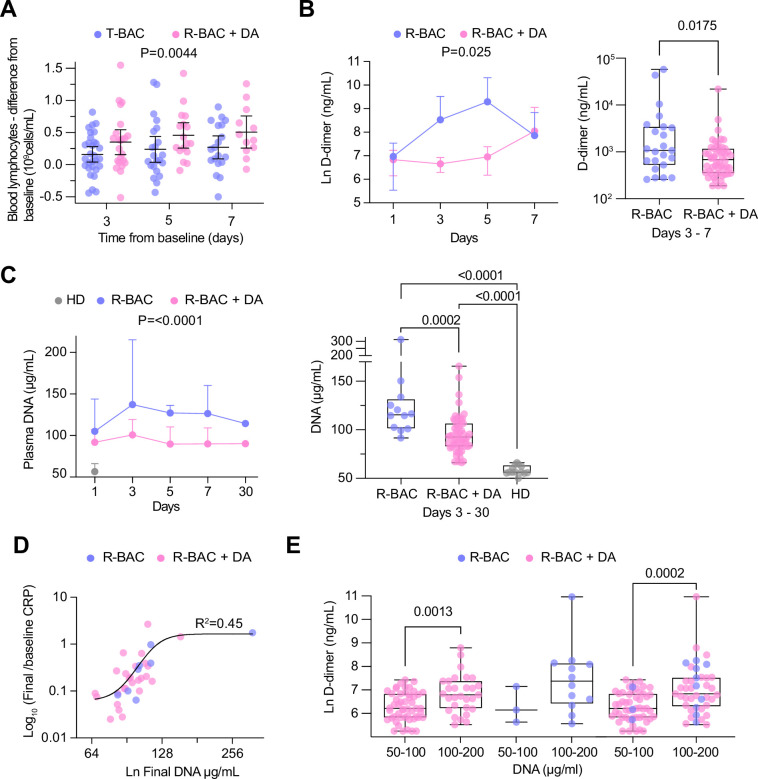
Results: We recruited 39 evaluable participants: 30 randomized to dornase alfa (R-BAC +DA), 9 randomized to BAC (R-BAC), and included 60 CC-BAC participants. Dornase alfa was well tolerated and reduced CRP by 33% compared to the combined BAC groups (T-BAC). Least squares (LS) mean post-dexamethasone CRP fell from 101.9 mg/L to 23.23 mg/L in R-BAC +DA participants versus a 99.5 mg/L to 34.82 mg/L reduction in the T-BAC group at 7 days; p=0.01. The anti-inflammatory effect of dornase alfa was further confirmed with subgroup and sensitivity analyses on randomised participants only, mitigating potential biases associated with the use of CC-BAC participants. Dornase alfa increased live discharge rates by 63% (HR 1.63, 95% CI 1.01-2.61, p=0.03), increased lymphocyte counts (LS mean: 1.08 vs 0.87, p=0.02) and reduced circulating cf-DNA and the coagulopathy marker D-dimer (LS mean: 570.78 vs 1656.96 μg/mL, p=0.004).
Conclusions: Dornase alfa reduces pathogenic inflammation in COVID-19 pneumonia, demonstrating the benefit of cost-effective therapies that target extracellular chromatin.
Funding: LifeArc, Breathing Matters, The Francis Crick Institute (CRUK, Medical Research Council, Wellcome Trust).
Clinical trial number: NCT04359654.
Keywords: COVID-19; DNA; DNase; NETs; dornase alfa; histone; immunology; inflammation; medicine; viruses.
© 2023, Porter et al.
Conflict of interest statement
JP, VS, ED, RE, MT, ND, IA, DH, DB, TC, JG, AW, HE, VJ, AL, TR, LL, EH, FK, BW, VB, VP No competing interests declared, JI, AF Employee of Exploristics, PL Employee of Target to Treatment Consulting Ltd
Figures
Update of
- doi: 10.1101/2022.04.14.22272888
- doi: 10.7554/eLife.87030.1
- doi: 10.7554/eLife.87030.2
- doi: 10.7554/eLife.87030.3
References
-
- Aramburu IV, Hoving D, Vernardis SI, Tin MCF, Ioannou M, Temkin MI, De Vasconcelos NM, Demichev V, Helbig ET, Lippert L, Stahl K, White M, Radbruch H, Ihlow J, Horst D, Chiesa ST, Deanfield JE, David S, Bode C, Kurth F, Ralser M, Papayannopoulos V. Functional proteomic profiling links deficient DNA clearance with increased mortality in individuals with severe COVID-19 pneumonia. Immunity. 2022;55:2436–2453. doi: 10.1016/j.immuni.2022.11.007. - DOI - PMC - PubMed
-
- Cui Z, Merritt Z, Assa A, Mustehsan H, Chung E, Liu S, Kumthekar A, Ayesha B, McCort M, Palaiodimos L, Baron S, Averbukh Y, Southern W, Arora S. Early and significant reduction in C-reactive protein levels after corticosteroid therapy is associated with reduced mortality in patients with COVID-19. Journal of Hospital Medicine. 2021;16:142–148. doi: 10.12788/jhm.3560. - DOI - PubMed
-
- Fisher J, Mohanty T, Karlsson CAQ, Khademi SMH, Malmström E, Frigyesi A, Nordenfelt P, Malmstrom J, Linder A. Proteome profiling of recombinant dnase therapy in reducing NETs and aiding recovery in COVID-19 patients. Molecular & Cellular Proteomics. 2021;20:100113. doi: 10.1016/j.mcpro.2021.100113. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
