

Opioid prescribing requirements to minimize unused medications after an emergency department visit for acute pain: a prospective cohort study
- PMID: 39009368
- PMCID: PMC11268147
- DOI: 10.1503/cmaj.231640
Opioid prescribing requirements to minimize unused medications after an emergency department visit for acute pain: a prospective cohort study
Abstract
Background: Unused opioid prescriptions can be a driver of opioid misuse. Our objective was to determine the optimal quantity of opioids to prescribe to patients with acute pain at emergency department discharge, in order to meet their analgesic needs while limiting the amount of unused opioids.
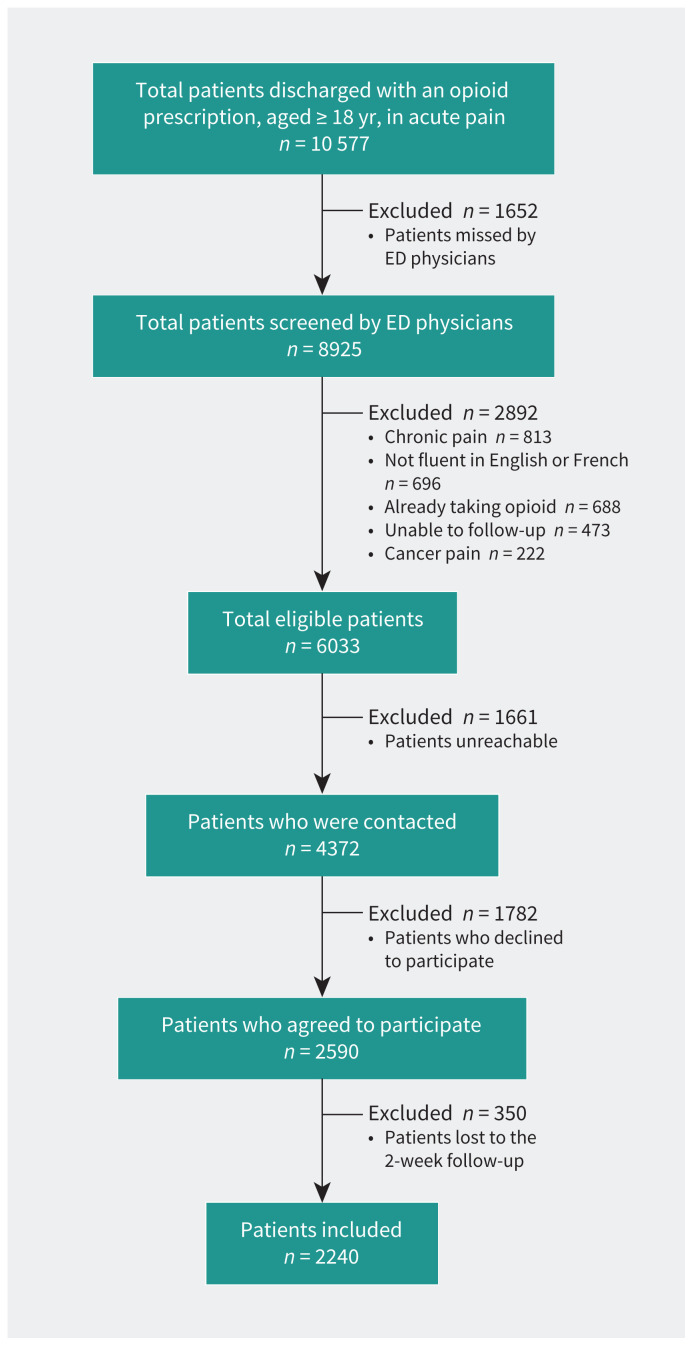
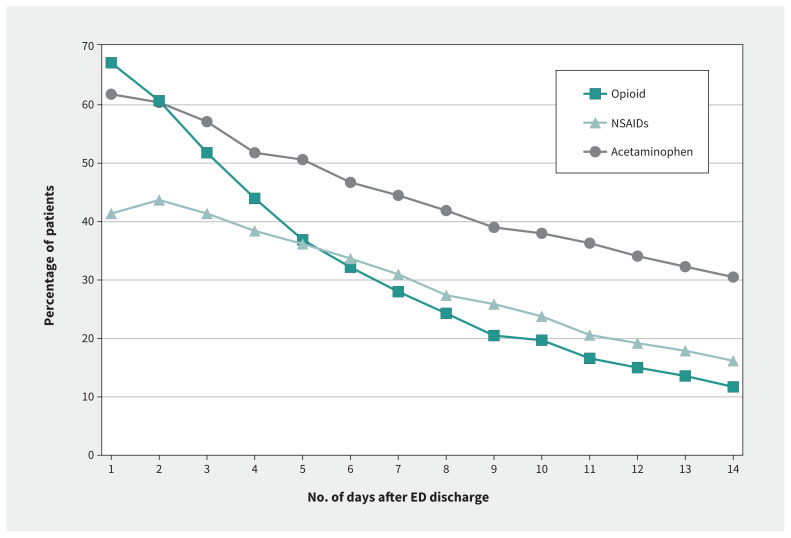
Methods: In a prospective, multicentre cohort study, we included consecutive patients aged 18 years and older with an acute pain condition present for less than 2 weeks who were discharged from emergency department with an opioid prescription. Participants completed a pain medication diary for real-time recording of quantity, doses, and names of all analgesics consumed during a 14-day follow-up period.
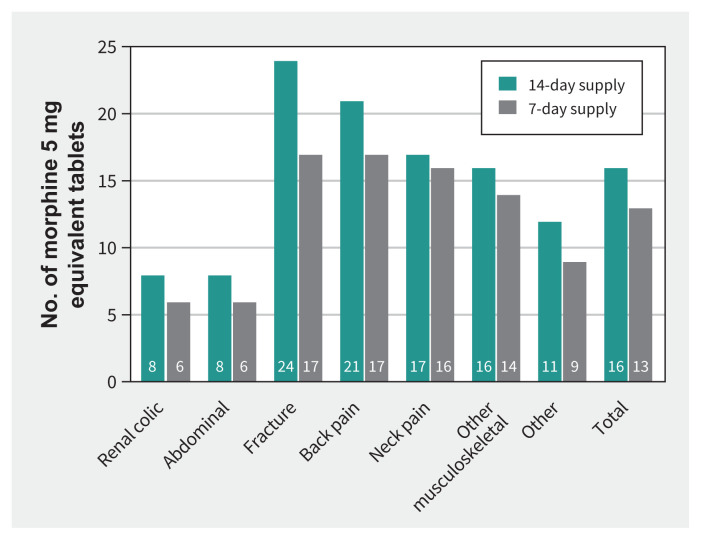
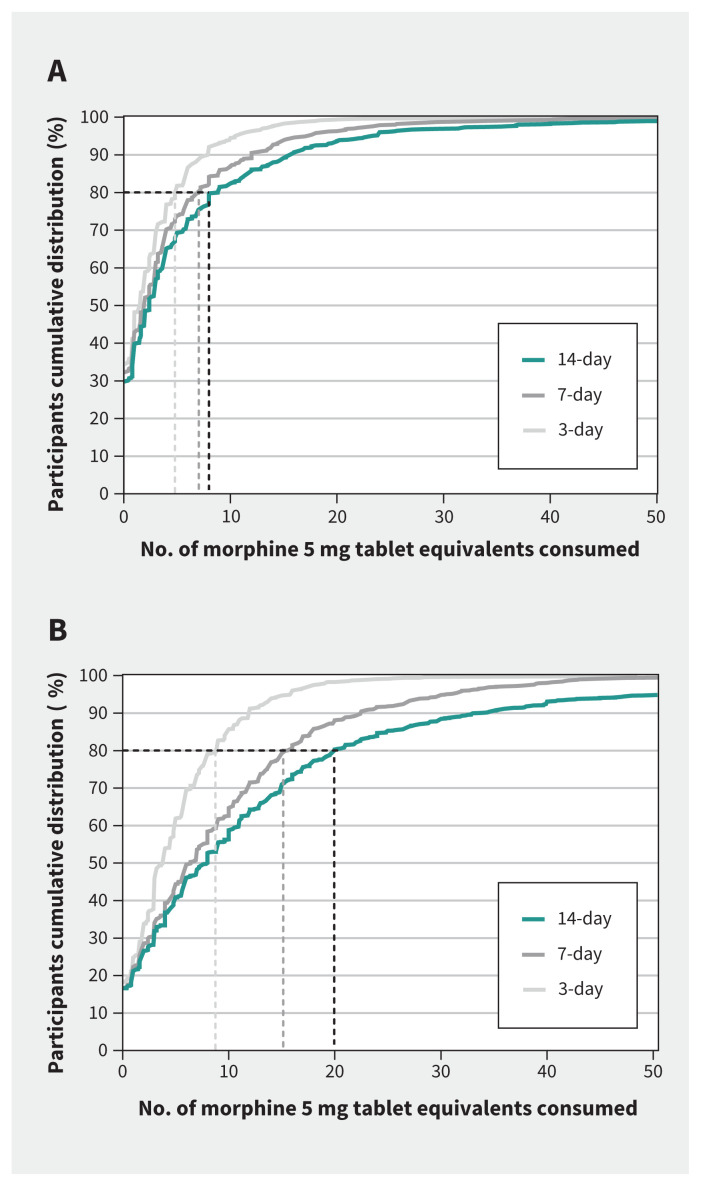
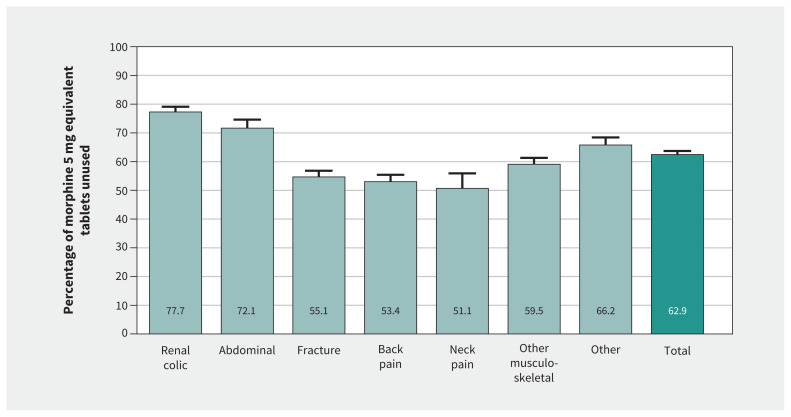
Results: We included 2240 participants, who had a mean age of 51 years; 48% were female. Over 14 days, participants consumed a median of 5 (quartiles, 1-14) morphine 5 mg tablet equivalents, with significant variation across pain conditions (p < 0.001). Most opioid tablets prescribed (63%) were unused. To meet the opioid need of 80% of patients for 2 weeks, we found that those experiencing renal colic or abdominal pain required fewer opioid tablets (8 morphine 5 mg tablet equivalents) than patients who had fractures (24 tablets), back pain (21 tablets), neck pain (17 tablets), or other musculoskeletal pain (16 tablets).
Interpretation: Two-thirds of opioid tablets prescribed at emergency department discharge for acute pain were unused, whereas opioid requirements varied significantly based on the cause of acute pain. Smaller, cause-specific opioid prescriptions could provide adequate pain management while reducing the risk of opioid misuse.
Trial registration: ClinicalTrials.gov, no. NCT03953534.
© 2024 CMA Impact Inc. or its licensors.
Conflict of interest statement
Competing interests:: Justin Yan reports receiving funding from the Spring 2021 Innovation Fund from the Academic Medical Organization of Southwestern Ontario, and the 2021 Internal Research Fund for Pilot Studies from the Lawson Health Research Institute. Dr. Yan has also served as the chair of the data safety monitoring boards of the RAFF4 Study and the REMOSYNCED Study, and vice-chair of the Canadian Association of the Emergency Physicians Research Committee. Jeffrey Perry reports receiving a peer review salary support grant from the Heart and Stroke Foundation of Ontario. Gilles Lavigne reports receiving consulting fees from Straumann Suisse related to a sleep bruxism device, and an oral appliance for sleep apnea from Panthera Dental. Dr. Lavigne is also a board member of the Canadian Academy of Health Sciences. No other competing interests were declared.
Figures
References
-
- Drug overdose death rates. Bethesda (MD): National Institute on Drug Abuse; 2023. Available: https://nida.nih.gov/research-topics/trends-statistics/overdose-death-rates (accessed 2023 Nov. 23).
-
- Opioid- and stimulant-related harms in Canada. Ottawa: Public Health Agency of Canada; modified 2024 Mar. 27. Available: https://health-infobase.canada.ca/substance-related-harms/opioids-stimul... (accessed 2023 Nov. 23)
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical