

Whole genome sequencing refines stratification and therapy of patients with clear cell renal cell carcinoma
- PMID: 39009593
- PMCID: PMC11250826
- DOI: 10.1038/s41467-024-49692-1
Whole genome sequencing refines stratification and therapy of patients with clear cell renal cell carcinoma
Abstract
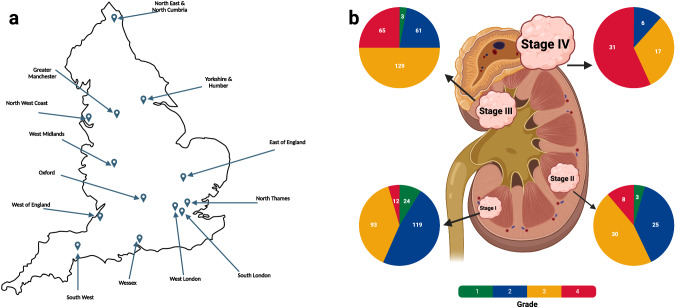
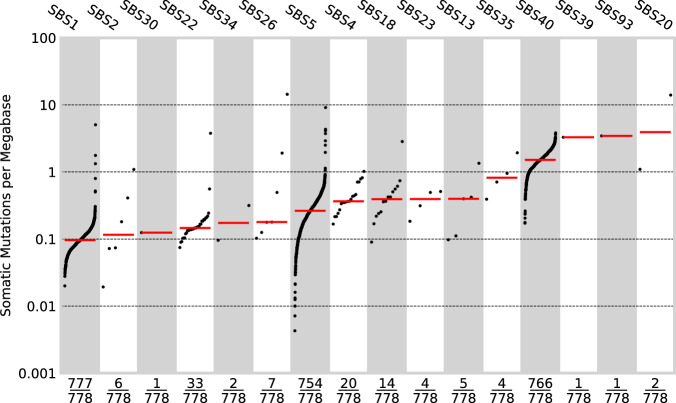
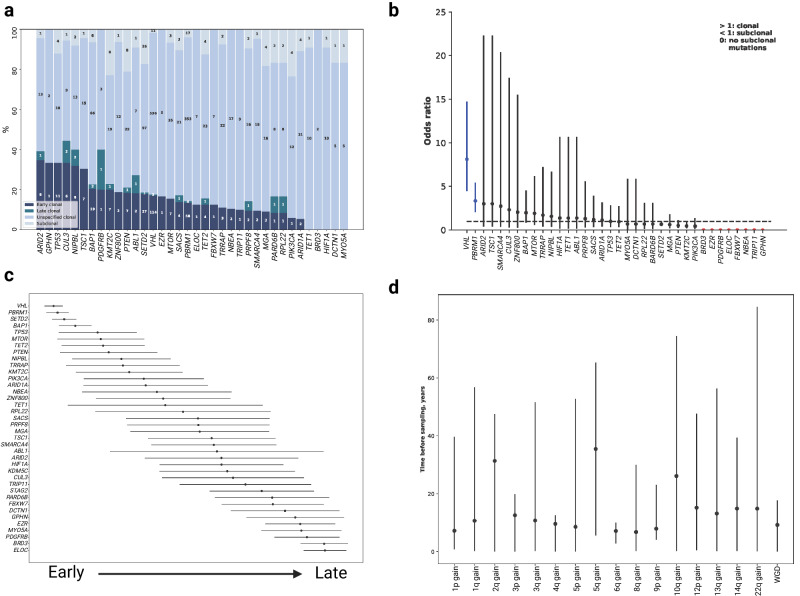
Clear cell renal cell carcinoma (ccRCC) is the most common form of kidney cancer, but a comprehensive description of its genomic landscape is lacking. We report the whole genome sequencing of 778 ccRCC patients enrolled in the 100,000 Genomes Project, providing for a detailed description of the somatic mutational landscape of ccRCC. We identify candidate driver genes, which as well as emphasising the major role of epigenetic regulation in ccRCC highlight additional biological pathways extending opportunities for therapeutic interventions. Genomic characterisation identified patients with divergent clinical outcome; higher number of structural copy number alterations associated with poorer prognosis, whereas VHL mutations were independently associated with a better prognosis. The observations that higher T-cell infiltration is associated with better overall survival and that genetically predicted immune evasion is not common supports the rationale for immunotherapy. These findings should inform personalised surveillance and treatment strategies for ccRCC patients.
© 2024. The Author(s).
Conflict of interest statement
S.T. has received speaking fees from Roche, AstraZeneca, Novartis and Ipsen. S.T. has the following patents filed: Indel mutations as a therapeutic target and predictive biomarker PCTGB2018/051892 and PCTGB2018/051893 and Clear Cell Renal Cell Carcinoma Biomarkers P113326GB. None of the other authors have a financial or non-financial conflict of interest.
Figures





Update of
-
Whole genome sequencing refines stratification and therapy of patients with clear cell renal cell carcinoma.Res Sq [Preprint]. 2023 Dec 6:rs.3.rs-3675752. doi: 10.21203/rs.3.rs-3675752/v1. Res Sq. 2023. Update in: Nat Commun. 2024 Jul 15;15(1):5935. doi: 10.1038/s41467-024-49692-1. PMID: 38106039 Free PMC article. Updated. Preprint.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
