

Consumer wearable devices for evaluation of heart rate control using digoxin versus beta-blockers: the RATE-AF randomized trial
- PMID: 39009776
- PMCID: PMC11271403
- DOI: 10.1038/s41591-024-03094-4
Consumer wearable devices for evaluation of heart rate control using digoxin versus beta-blockers: the RATE-AF randomized trial
Abstract
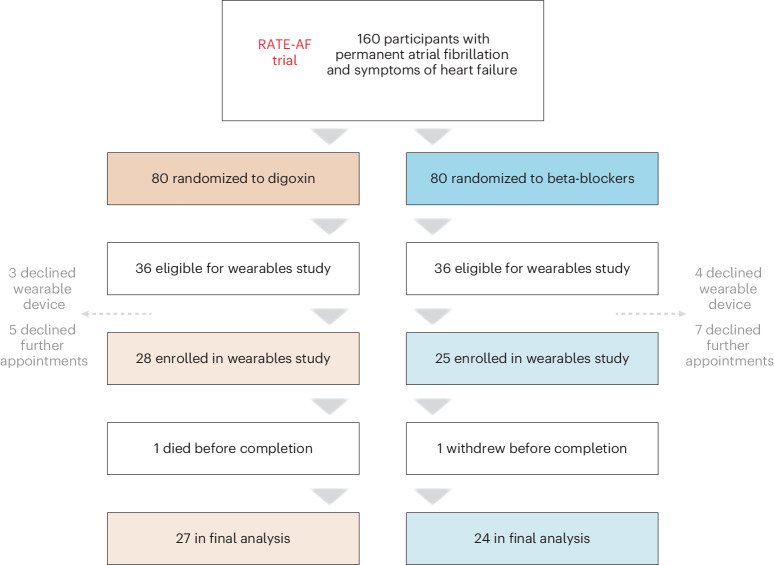
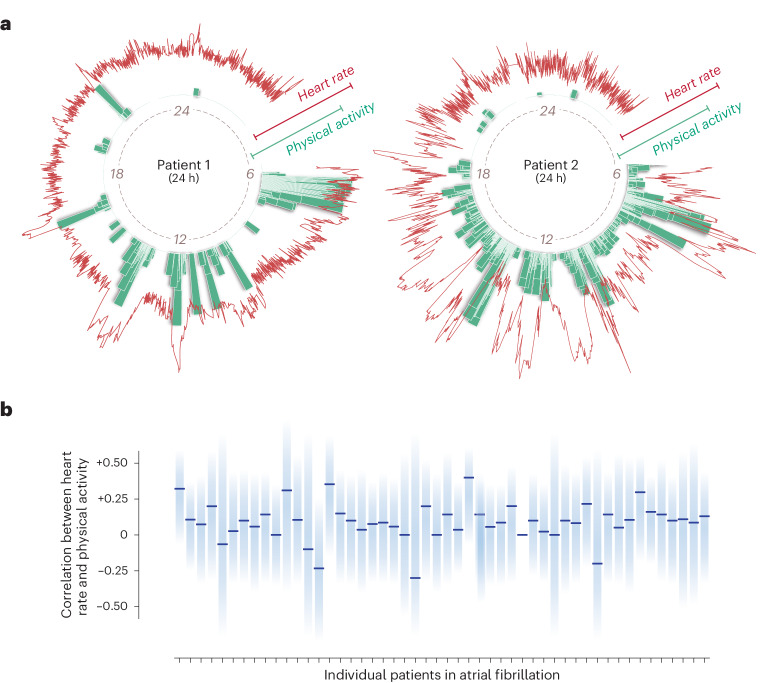
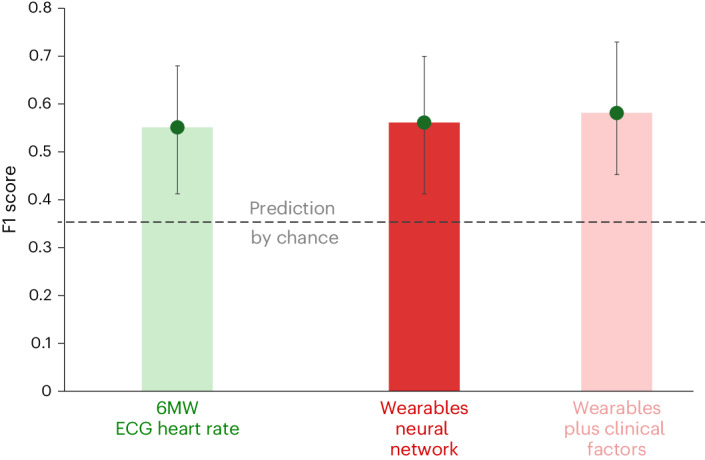
Consumer-grade wearable technology has the potential to support clinical research and patient management. Here, we report results from the RATE-AF trial wearables study, which was designed to compare heart rate in older, multimorbid patients with permanent atrial fibrillation and heart failure who were randomized to treatment with either digoxin or beta-blockers. Heart rate (n = 143,379,796) and physical activity (n = 23,704,307) intervals were obtained from 53 participants (mean age 75.6 years (s.d. 8.4), 40% women) using a wrist-worn wearable linked to a smartphone for 20 weeks. Heart rates in participants treated with digoxin versus beta-blockers were not significantly different (regression coefficient 1.22 (95% confidence interval (CI) -2.82 to 5.27; P = 0.55); adjusted 0.66 (95% CI -3.45 to 4.77; P = 0.75)). No difference in heart rate was observed between the two groups of patients after accounting for physical activity (P = 0.74) or patients with high activity levels (≥30,000 steps per week; P = 0.97). Using a convolutional neural network designed to account for missing data, we found that wearable device data could predict New York Heart Association functional class 5 months after baseline assessment similarly to standard clinical measures of electrocardiographic heart rate and 6-minute walk test (F1 score 0.56 (95% CI 0.41 to 0.70) versus 0.55 (95% CI 0.41 to 0.68); P = 0.88 for comparison). The results of this study indicate that digoxin and beta-blockers have equivalent effects on heart rate in atrial fibrillation at rest and on exertion, and suggest that dynamic monitoring of individuals with arrhythmia using wearable technology could be an alternative to in-person assessment. ClinicalTrials.gov identifier: NCT02391337 .
© 2024. The Author(s).
Conflict of interest statement
All authors have completed the International Committee of Medical Journal Editors uniform disclosure form and declare: S.K.G. reports funding through the BigData@Heart Innovative Medicines Initiative (grant no.116074). K.V.B. reports grants from the National Institute for Health Research (NIHR) (grant no. CDF-2015-08-074 RATE-AF) during conduct of the study; and has been awarded a British Heart Foundation (BHF) Career Development Research Fellowship (FS/CDRF/21/21032). A.J.C. reports personal fees from Medtronic, Boston Scientific, Abbott, Bayer, Daiichi-Sankyo, Pfizer/BMS, Sanofi and Menarini; all outside the submitted work. D.K. reports grants from the NIHR (grant nos. CDF-2015-08-074 RATE-AF; NIHR130280 DaRe2THINK; NIHR132974 D2T-NeuroVascular; NIHR203326 Biomedical Research Centre), the BHF (grant nos. PG/17/55/33087, AA/18/2/34218 and FS/CDRF/21/21032), the European Union/European Federation of Pharmaceutical Industries and Associations Innovative Medicines Initiative (BigData@Heart, grant no. 116074), European Union Horizon and UK Research and Innovation (HYPERMARKER, grant no. 101095480), UK National Health Service—Data for R&D—Subnational Secure Data Environment programme, UK Department for Business, Energy & Industrial Strategy Regulators Pioneer Fund, the Cook & Wolstenholme Charitable Trust, and the European Society of Cardiology supported by educational grants from Boehringer Ingelheim/BMS-Pfizer Alliance/Bayer/Daiichi-Sankyo/Boston Scientific, the NIHR/University of Oxford Biomedical Research Centre and BHF/University of Birmingham Accelerator Award (STEEER-AF). In addition, D.K. has received research grants and advisory board fees from Bayer, Amomed and Protherics Medicines Development; all outside the submitted work. The remaining authors declare no competing interests.
Figures



References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
