

Management of Proximal Hamstring Injuries: Non-operative and Operative Treatment
- PMID: 39009901
- PMCID: PMC11335994
- DOI: 10.1007/s12178-024-09911-0
Management of Proximal Hamstring Injuries: Non-operative and Operative Treatment
Abstract
Purpose of review: To evaluate the current evidence and literature on treatment options for proximal hamstring injuries.
Recent findings: Patients with 3-tendon complete tears with greater than 2 cm of retraction have worse outcomes and higher complication rates compared to those with less severe injuries. Endoscopic and open proximal hamstring repair both have favorable patient reported outcomes at 5-year follow up. Proximal hamstring repair in patients who are male, with isolated semimembranosus injury, and have proximal hamstring free tendon rupture are more likely to have earlier return to sports. The Parisian Hamstring Avulsion Score (PHAS) is a validated patient-reported outcome measure to predict return to sports. Proximal hamstring injuries may occur in both elite and recreational athletes and may present with varying degrees of chronicity and severity. Injuries occur most commonly during forceful eccentric contraction of the hamstrings and often present with ischial tuberosity tenderness, ecchymosis, and hamstring weakness. Treatment decision-making is dictated by the tendons involved and chronicity. Many proximal hamstring injuries can be successfully treated with non-surgical measures. However, operative treatment of appropriately indicated proximal hamstring tendon injuries can result in significantly better functional outcomes and faster and more reliable return to sports compared to nonoperative treatment. Both endoscopic and open surgical repair techniques show high satisfaction levels and excellent patient-reported outcomes at short- and mid-term follow-up. Postoperative rehabilitation protocols vary across the literature and ongoing study is needed to clarify the optimal program, though emphasis on eccentric hamstring strengthening may be beneficial.
Keywords: Endoscopic repair; Hamstring; Open repair; Tendon injury; Treatment outcomes.
© 2024. The Author(s), under exclusive licence to Springer Science+Business Media, LLC, part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Figures






References
-
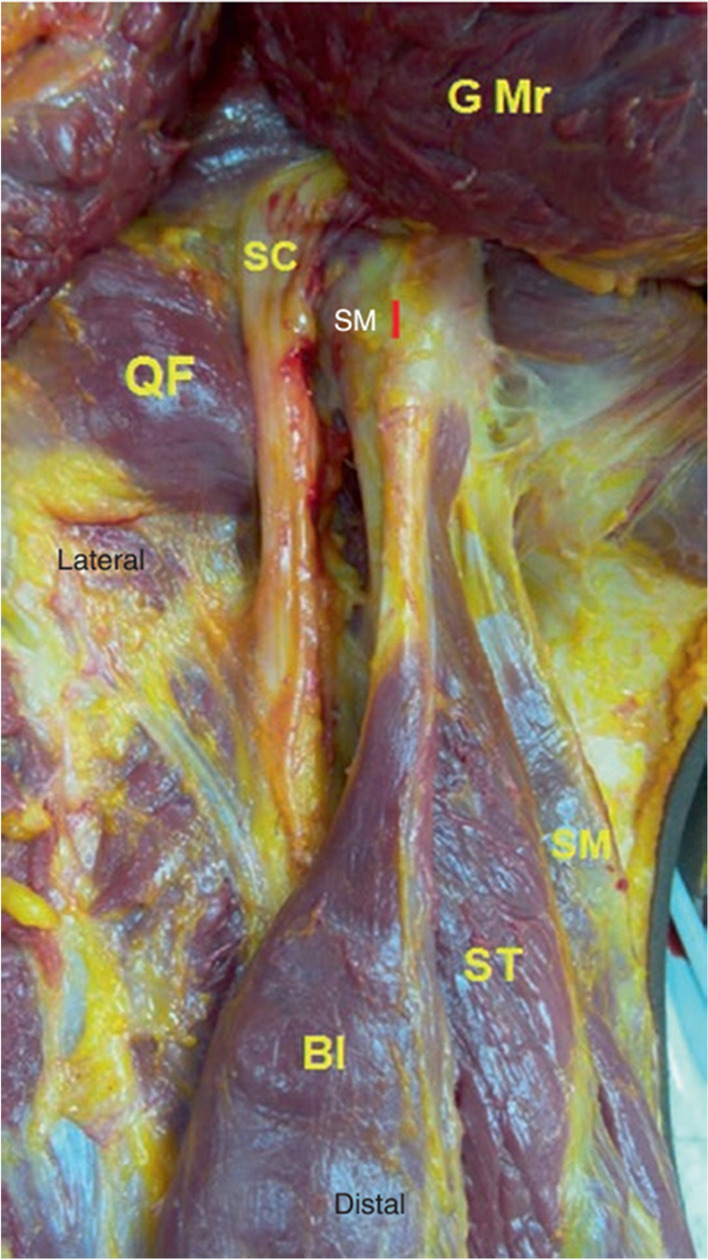
- Miller SL, Gill J, Webb GR. The proximal origin of the hamstrings and surrounding anatomy encountered during repair. A cadaveric study [published correction appears in J Bone Joint Surg Am. 2007 Mar;89(3):637]. J Bone Joint Surg Am. 2007;89(1):44–8. 10.2106/JBJS.F.00094. 10.2106/JBJS.F.00094 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
