

Integrated clustering of multiple immune marker trajectories reveals different immunotypes in severely injured patients
- PMID: 39010113
- PMCID: PMC11247757
- DOI: 10.1186/s13054-024-04990-4
Integrated clustering of multiple immune marker trajectories reveals different immunotypes in severely injured patients
Abstract
Background: The immune response of critically ill patients, such as those with sepsis, severe trauma, or major surgery, is heterogeneous and dynamic, but its characterization and impact on outcomes are poorly understood. Until now, the primary challenge in advancing our understanding of the disease has been to concurrently address both multiparametric and temporal aspects.
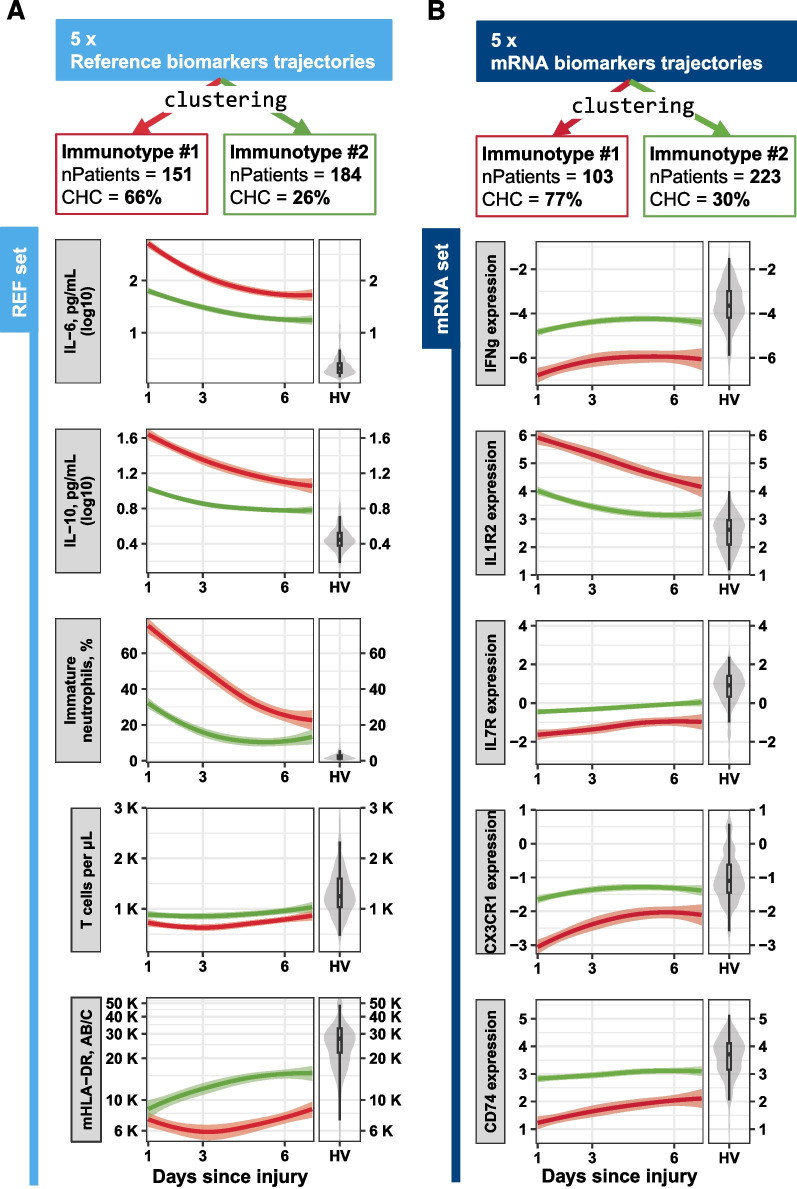
Methods: We used a clustering method to identify distinct groups of patients, based on various immune marker trajectories during the first week after admission to ICU. In 339 severely injured patients, we initially longitudinally clustered common biomarkers (both soluble and cellular parameters), whose variations are well-established during the immunosuppressive phase of sepsis. We then applied this multi-trajectory clustering using markers composed of whole blood immune-related mRNA.
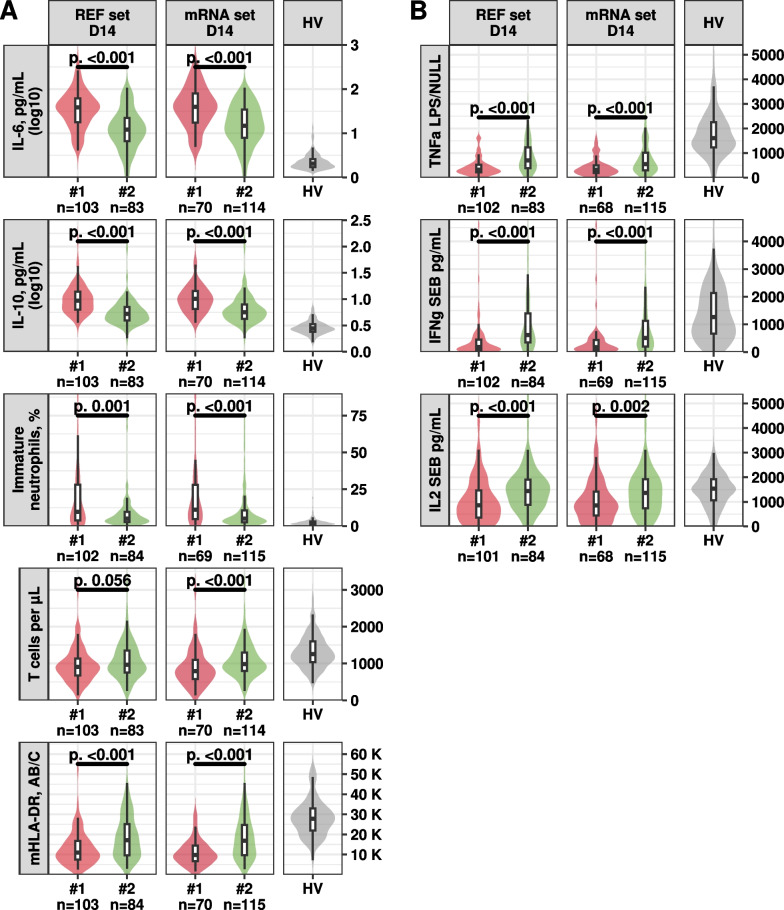
Results: We found that both sets of markers revealed two immunotypes, one of which was associated with worse outcomes, such as increased risk of hospital-acquired infection and mortality, and prolonged hospital stays. This immunotype showed signs of both hyperinflammation and immunosuppression, which persisted over time.
Conclusion: Our study suggest that the immune system of critically ill patients can be characterized by two distinct longitudinal immunotypes, one of which included patients with a persistently dysregulated and impaired immune response. This work confirms the relevance of such methodology to stratify patients and pave the way for further studies using markers indicative of potential immunomodulatory drug targets.
Keywords: Critical illness; Immune markers; Immune response; Immunosuppression; Longitudinal study; Patient stratification; Sepsis; Trajectory; Transcriptomic.
© 2024. The Author(s).
Conflict of interest statement
MB, EP, JFL, AF, KBP and JT are employees of bioMérieux SA, an in vitro diagnostic company. TR, FV, DMB and GM are employees of Hospices Civils de Lyon. MB, EP, JFL, AF, KBP, JT, FV, LK, and GM work in a joint research unit, co funded by the Hospices Civils de Lyon and bioMérieux.
Figures


References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
